
Introduction
Hospitals discharge patients every day with detailed dietary instructions and no practical way to follow them. A patient with congestive heart failure gets a sodium-restricted diet sheet. A dialysis patient receives a low-potassel meal guide. Then they go home — often alone, often food-insecure — and eat whatever is available.
The gap between clinical guidance and real-world nutrition drives preventable readmissions. Food insecurity is associated with a 47% increase in hospitalizations and a 54% increase in days hospitalized among affected patients.
Among patients with heart failure specifically, dietary noncompliance is implicated in 26.4% of 30-day readmissions.
Medically tailored meal (MTM) delivery addresses this directly. MTMs are clinically prescribed, dietitian-designed meals delivered to patients at home — a healthcare intervention with measurable outcomes, distinct from consumer meal subscriptions.
This article covers:
- Who benefits most from MTM programs
- What the clinical evidence shows
- How coverage and reimbursement work
- What it takes to coordinate MTM delivery within a hospital's discharge workflow
Key Takeaways
- MTMs are clinically prescribed and dietitian-designed for specific conditions — not general healthy eating programs
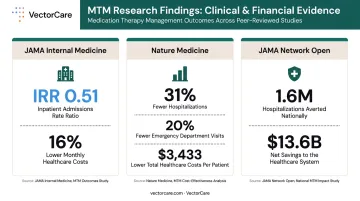
- Research links MTM programs to 31% fewer hospitalizations and $3,433 lower total healthcare costs per patient
- Medicare Advantage is the primary coverage pathway — 57% of individual MA plans offer meal benefits in 2026
- Effective MTM delivery requires integration into discharge workflows alongside home health, DME, and transport
What Are Medically Tailored Meals — and How Do They Differ from Regular Meal Delivery?
The Clinical Definition
The Food Is Medicine Coalition (FIMC) defines medically tailored meals as meals for people with severe, chronic, or complex illness, tied to a healthcare referral and a Registered Dietitian Nutritionist (RDN) assessment. MTMs are a clinical intervention — prescribed, not purchased.
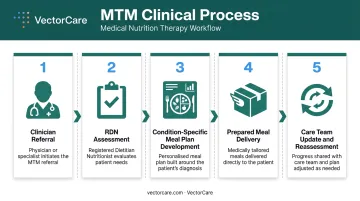
The process involves:
- A clinician refers the patient to an MTM program
- An RDN assesses the patient's diagnosis, comorbidities, and dietary restrictions
- Develop a condition-specific meal plan with precise macro and micronutrient targets
- Fully prepared, ready-to-heat meals are delivered at regular intervals
- The care team receives ongoing updates, and the meal plan is reassessed as the patient's condition changes
Who MTMs Are Designed For
The conditions most commonly addressed by MTM programs include:
- Type 2 diabetes — carbohydrate-controlled meals calibrated to glycemic management
- Chronic kidney disease (CKD) — low-potassium, low-phosphorus, protein-adjusted meals
- Congestive heart failure — sodium-restricted, fluid-conscious meal planning
- HIV/AIDS — high-protein, nutrient-dense meals supporting immune function
- Cancer — meals designed around treatment-related nutritional challenges
Standard consumer meal delivery services, including subscription kits and "health-focused" direct-to-consumer brands, fail these patients. Wrong sodium levels, insufficient protein, no renal restrictions, no clinical oversight. A CKD patient eating a "healthy" consumer meal with standard potassium levels can trigger a hospitalization.
MTMs vs. "Medically Friendly" Consumer Meals
Some services market themselves as condition-appropriate without meeting the clinical bar. The distinction matters:
| Feature | True MTM Program | Consumer "Healthy" Meal Service |
|---|---|---|
| Clinical referral required | Yes | No |
| RDN assessment and oversight | Yes | No |
| Condition-specific nutrition targets | Yes | General guidelines only |
| Care team integration | Yes | No |
| Outcomes tracking | Yes | No |
| Patient selects from menu | No | Yes |
True MTM programs are prescribed and delivered. The patient does not browse a menu.
Which Patients Benefit Most from Medically Tailored Meal Delivery?
High-Priority Populations
MTM programs deliver the most value for patients who combine clinical complexity with real-world barriers to consistent nutrition:
- Recently discharged patients with diet-sensitive chronic conditions in the high-risk 30-day window
- Food-insecure patients — food insecurity reaches 50.8% among urban public hospital ED patients and 62.8% among frequent ED users (4+ visits per year)
- Elderly patients who face mobility limitations, cognitive challenges, or live alone
- Transitional care patients moving from hospital to home without family support
Conditions With the Strongest MTM Evidence
The strongest clinical evidence covers:
- CKD and end-stage renal disease — a Massachusetts MTM evaluation found $12,312 net savings per CKD patient and significant reductions in total cost of care
- Congestive heart failure — a randomized trial found exploratory reduction in HF-related hospitalizations (aHR 0.53, 95% CI 0.33–0.88) among MTM recipients
- Type 2 diabetes — a randomized crossover trial found higher Healthy Eating Index scores and lower food insecurity during MTM periods
- HIV/AIDS — studies report lower hospitalization odds and improved antiretroviral therapy adherence
The SDOH Dimension
MTM delivery is one of the few interventions that addresses social determinants of health (SDOH) directly, rather than referring patients to resources they may not access. Many patients who need MTMs lack:
- Transportation to grocery stores
- Physical ability to cook
- Household members who can assist with meal preparation
- Financial resources for condition-appropriate foods
These gaps explain why MTM programs are most effective when embedded in care settings that already coordinate services at home — where the logistics of delivery, not just the clinical order, determine whether a patient actually benefits.
Settings Where MTMs Are Most Often Implemented
- PACE organizations — which coordinate comprehensive medical and social services for frail older adults and commonly bundle meal delivery with transportation and home health
- Medicare Advantage plans — which have supplemental benefit flexibility to cover MTMs
- Home health patients — who are already receiving services at home, making MTM delivery a natural addition
- SNFs — where MTM programs support transitional care and reduce readmission risk before patients return home
The Clinical Evidence: How MTMs Reduce Readmissions and Improve Outcomes
What the Research Shows
Three peer-reviewed studies make the clinical case for MTMs. Key findings:
- A cohort study published in JAMA Internal Medicine found MTM receipt associated with fewer inpatient admissions (IRR 0.51), fewer skilled nursing admissions (IRR 0.28), and 16% lower monthly medical costs (approximately $753 per month) among medically and socially complex adults
- A Nature Medicine evaluation of 1,866 MTM recipients found 31% fewer hospitalizations, 20% fewer ED visits, and $3,433 lower total healthcare costs — with cost reductions offsetting 98% of program costs
- A national simulation in JAMA Network Open estimated that expanding MTM access nationally could avert 1.6 million hospitalizations and generate $13.6 billion in net savings in year one
Why MTMs Interrupt the Readmission Cycle
Poor nutrition after discharge does not just cause discomfort. It accelerates disease progression, weakens immune response, impairs medication efficacy, and prolongs recovery. Heart failure patients eating high-sodium meals at home face worsening fluid retention. CKD patients with uncontrolled potassium intake run a higher risk of cardiac events.
MTMs interrupt this cycle by ensuring that every meal the patient receives between discharge and their next clinical encounter is calibrated to their condition. The 30-day post-discharge window — when readmission risk is highest — is also when unsupported patients are most likely to experience nutritional noncompliance.
Cost-Effectiveness for Payers and Health Systems
A Health Affairs state-level model estimated that MTM coverage produces net cost savings in 49 states, with first-year per-patient savings reaching $6,299 in some states and the lowest number-needed-to-treat to avert one hospitalization at 2.3 patients in Maryland.
For value-based care programs and Medicare Advantage plans tracking total cost of care, MTMs are one of the few supplemental benefits where the return on investment has been modeled and, in some cases, observed in real-world pilots. At a number-needed-to-treat of 2.3, few interventions at this cost level deliver comparable hospitalization avoidance.
Understanding Coverage and Payment for Medically Tailored Meal Delivery
Traditional Medicare (Parts A, B, D)
Traditional fee-for-service Medicare does not cover MTM meal delivery as a standalone benefit. Part B covers Medical Nutrition Therapy services (counseling by an RDN) for patients with diabetes, kidney disease, or post-transplant conditions, but that covers the clinical consultation only — not the meals themselves.
For patients who need the meals themselves covered, Medicare Advantage is where most pathways exist.
The Medicare Advantage Pathway
Medicare Advantage is the primary coverage channel for MTMs. The Bipartisan Budget Act of 2018 expanded MA plans' authority to offer non-primarily health-related supplemental benefits for chronically ill enrollees, including home-delivered meals.
The Medicare Advantage Pathway
Key data points for 2026:
- 57% of individual MA plans offer meal benefits
- 66% of Special Needs Plans (SNPs) offer meal benefits
- 85% of SNPs offer food and produce benefits under Special Supplemental Benefits for the Chronically Ill (SSBCI)
Coverage varies by plan. Patients and care coordinators should verify specific benefits, quantity limits, and eligibility criteria with each MA plan directly.
Medicaid and State-Level Pathways
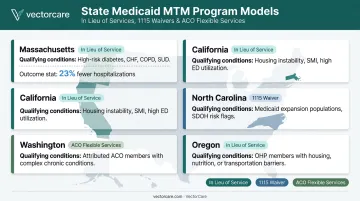
Beyond Medicare Advantage, several states have built their own Medicaid pathways — often with stricter clinical eligibility criteria tied to specific diagnoses or utilization history. Examples:
- New York — designated MTMs as a State Initiated In Lieu of Service for patients with cancer, diabetes, heart failure, or HIV/AIDS who had at least one hospitalization in the prior year
- Oregon — established MTM clinical eligibility criteria under its HRSN 1115 waiver
- Massachusetts — delivered nutrition supports including MTMs through its Flexible Services Program across 17 ACOs, associated with 23% fewer hospitalizations and 13% fewer ED visits
- California — CalAIM community supports pathway includes food and nutrition interventions
- North Carolina — Healthy Opportunities Pilot includes food and nutrition access supports
Medicaid eligibility for MTMs varies by state, waiver type, and managed care contract. A care coordinator familiar with local waiver structures is the most reliable guide to what's actually available.
Building an Effective MTM Coordination Strategy for Health Systems
The Real Operational Challenge
Sourcing an MTM provider is the easy part. The harder problem is integration. When a patient is discharged, they typically need multiple services initiated simultaneously: home health, DME, transportation, follow-up appointments, and — for diet-sensitive conditions — medically tailored meals. Each of these services has its own vendor network, its own scheduling system, and its own communication process.
Most hospitals handle these sequentially. A case manager arranges the ride home, then calls a DME supplier, then refers to a home health agency, then — if the system even has an MTM program — contacts a meal delivery provider. By the time the patient's meal delivery is set up, the highest-risk days post-discharge have already passed.
Where Coordination Breaks Down
Common failure patterns include:
- Patients discharged with dietary instructions but no meal delivery arranged before leaving the facility
- MTM referral handled by a different team than home health and transport, with no shared visibility
- No system tracking whether the patient received meals, attended follow-up, or had their equipment delivered
- Providers across service types receiving incomplete patient information because it was entered separately into each system
These are logistics failures. And they are solvable with the right infrastructure.
How Unified Logistics Platforms Close the Gap
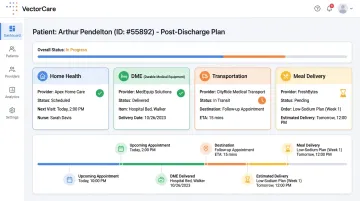
Health systems that coordinate post-discharge services through a single logistics infrastructure reduce the delays and communication failures that drive readmissions. Rather than initiating each service through a separate workflow, a unified platform allows a case manager to trigger home health scheduling, DME procurement, transportation, and meal delivery simultaneously — from within the clinical workflow.
Platforms like VectorCare unify post-discharge patient services — home health coordination, DME delivery, transport, and meal delivery — through one intelligent ecosystem. The key capabilities that matter for MTM integration are:
- Single-workflow initiation — all services triggered from one interface, embedded in the EHR
- Real-time status tracking — visibility into whether each service has been confirmed, dispatched, and delivered
- Vendor network management — credentialed providers across service types managed within one system
- EHR integration — automatic patient data pull eliminating duplicate data entry across service requests
For health systems in value-based care arrangements or serving Medicare Advantage populations, this coordination infrastructure directly determines whether MTM reaches patients during the highest-risk days post-discharge — not days later.
Frequently Asked Questions
Will Medicare pay for meal delivery?
Traditional Medicare (Parts A, B, and D) generally does not cover home-delivered meals as a standalone benefit. Medicare Advantage plans have more flexibility — 57% of individual MA plans offer meal benefits in 2026. Patients should check their specific plan documents or call their plan's member services line.
What is the best meal delivery service for elderly people?
For elderly patients with chronic conditions, clinically prescribed MTM programs are the appropriate choice, not consumer meal services. Programs developed with RDN oversight and condition-specific nutrition targets are built for this population's medical needs in ways that general delivery services cannot match.
Is there a meal plan for just one person?
Yes. MTM programs are designed for individual patients and delivered as single-serve, fully prepared meals. Unlike household meal kits, MTMs are calibrated to one patient's specific clinical profile — portion sizes, nutrient targets, and restrictions are all individualized.
What conditions qualify for medically tailored meals?
The most common qualifying conditions are diabetes, chronic kidney disease, congestive heart failure, HIV/AIDS, and cancer. Some programs include additional diet-sensitive conditions. Eligibility depends on the specific program, payer, and state.
How do medically tailored meals differ from regular meal delivery?
MTMs are clinically prescribed, designed by registered dietitians for a specific diagnosis, and coordinated with the patient's care team. Consumer meal services, including "healthy" options, lack clinical prescription, condition-specific nutrition design, and outcomes tracking.
Can medically tailored meals reduce hospital readmissions?
Yes. A Nature Medicine study found 31% fewer hospitalizations among MTM recipients. The effect is strongest for patients with diet-sensitive conditions in the 30-day post-discharge window, when nutritional noncompliance most directly triggers clinical deterioration.