Introduction
Despite 99.4% of U.S. non-federal acute care hospitals adopting certified EHRs as of 2024, patient data still fails to follow patients when it matters most.
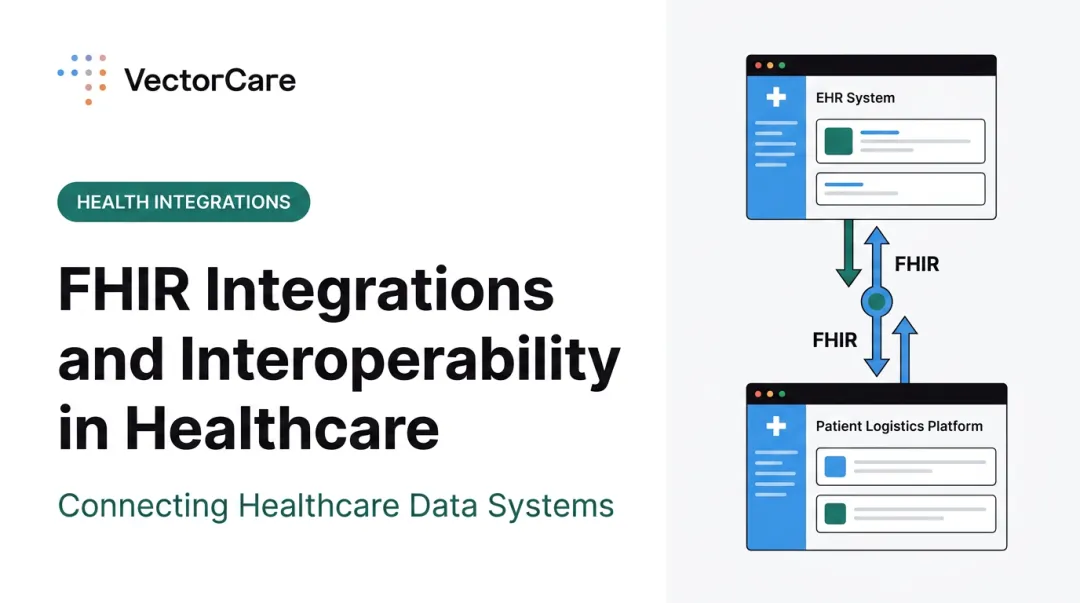
A care coordinator initiating a patient transfer calls the receiving facility, faxes clinical notes, manually re-enters demographics into a transport request, then calls again to confirm the pickup. The EHR sits open on a second screen — full of the information needed — but the transport system can't read it.
That gap is the EHR integration problem. Hospitals have digital records. What they often lack is any connection between those records and the downstream systems that move patients through the care continuum.
The following breaks down what EHR integration actually means, which standards govern it, where implementation breaks down, and why patient logistics remains one of its most consequential gaps.
What Is EHR Integration and Why Does It Matter in Digital Health?
EHR integration connects an electronic health record system to external software, platforms, or devices so patient data flows automatically between them. No manual re-entry. No fax-based record sharing. No duplicate documentation across systems.
The problem it solves is real and measurable. According to ONC data, only 43% of hospitals routinely engaged in all four interoperability domains — sending, receiving, finding, and integrating patient data — as of 2023.
The downstream gaps are just as stark. NCQA reports discharge summaries reach primary care within 48 hours only 55% of the time, diagnostic results are missing 40% of the time, and pending test results are absent 75% of the time.
Three Integration Approaches
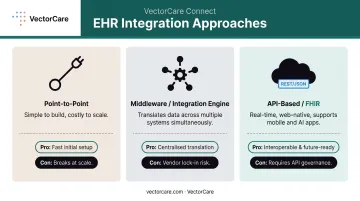
Healthcare organizations typically connect systems through one of three methods:
- Point-to-point connections: Direct links between two specific systems. Simple to build, expensive to maintain as the number of connections scales.
- Middleware / integration engines: Platforms that translate data between multiple systems simultaneously, acting as a central hub for message routing.
- API-based integrations (FHIR): Modern, web-native connections that support real-time data access for mobile apps, patient-facing tools, and AI-driven applications.
Why Federal Policy Has Made This Urgent
EHR integration is no longer just a competitive advantage — it's a compliance requirement:
- 21st Century Cures Act: Makes electronic health information sharing the expected norm and prohibits information blocking by providers and health IT developers
- ONC HTI-1 Final Rule (effective March 2024): Adopts USCDI Version 3 as the certification baseline by January 2026
- CMS-0057-F: Requires FHIR-based prior authorization APIs, with key provisions taking effect by January 2027
The global healthcare interoperability solutions market is projected to grow from USD $5.61B in 2026 to USD $9.57B by 2031 at 11.27% CAGR — driven largely by these regulatory pressures.
EHR vs. EMR: A Practical Distinction
That market growth reflects a broader shift in how healthcare organizations think about data ownership — and it starts with understanding what kind of system they're actually running.
The terms overlap in practice, but the functional distinction matters. EMR systems are designed for a single provider's internal use — records that don't leave the practice. EHR systems are built to exchange data across multiple providers and care settings. Most hospitals use EHRs precisely because patient data must travel beyond any one facility.
Key EHR Integration Standards: HL7, FHIR, and SMART on FHIR
HL7 v2: The Workhorse That Won't Retire
HL7 (Health Level Seven) v2 remains the most widely used health information exchange standard in the U.S. — the National Library of Medicine reports 95% of U.S. healthcare organizations use it. It handles the operational backbone of hospital data exchange: ADT (admission, discharge, transfer) events, lab orders, lab results, and billing messages.
More than 80% of Health Information Organizations routinely send and receive HL7 v2 messages. It's not elegant by modern standards, but it's deeply embedded in hospital workflows and isn't going away.
What Is FHIR and How Does It Differ from HL7?
FHIR (Fast Healthcare Interoperability Resources) is HL7's modern standard — but architecturally, they work in fundamentally different ways. Where HL7 v2 uses message-based formats over proprietary pipes, FHIR uses REST APIs, JSON, and the same web technologies that power consumer applications.
That distinction matters for what FHIR can support:
- Mobile and patient-facing applications
- Real-time data access at the point of care
- AI-driven clinical tools
- Third-party app ecosystems embedded within EHRs
By 2022, ONC reported that 9 in 10 hospitals used APIs for patient data access, with 67% using FHIR APIs — up 12 percentage points from 2021. Federal rules now mandate FHIR R4.0.1 as the API base standard under 45 CFR 170.215.
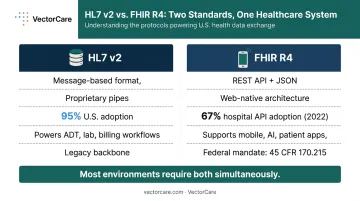
The key operational reality: most healthcare environments need both simultaneously. HL7 v2 keeps legacy hospital workflows running. FHIR powers modern digital health applications layered on top. Organizations that support only one will have significant gaps.
What Is SMART on FHIR and Why Does It Matter?
FHIR enables data exchange, but it doesn't define how third-party apps authenticate or launch inside an EHR. That's what SMART on FHIR solves. It's a framework that lets external applications open securely within the EHR interface — pre-populated with patient context, authenticated through standardized protocols, with no separate login or manual patient lookup required.
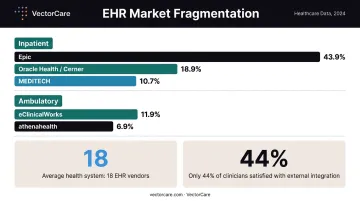
This is now the standard for EHR-embedded application development, particularly within Epic's ecosystem. Epic holds 43.9% of the U.S. inpatient hospital EHR market, making its App Showroom the largest app distribution channel in U.S. healthcare IT.
VectorCare, in partnership with Priority Dispatch Corp, launched a Medical Transfer Protocol SMART on FHIR App on the Epic Showroom — enabling care coordinators to initiate patient transport workflows directly from within Epic, with patient data automatically pulled into the transport request. The practical outcome:
- Transport requests that previously required phone calls and manual re-entry now complete in under a minute
- Care coordinators never leave the clinical workflow to initiate or track a transfer
- Patient data flows directly from Epic into the logistics request — no duplicate entry, no transcription errors
Common EHR Integration Challenges
Vendor Fragmentation
No single EHR dominates the entire U.S. market. Epic leads inpatient at 43.9%, followed by Oracle Health/Cerner at 18.9% and MEDITECH at 10.7%. In ambulatory settings, eClinicalWorks holds 11.9% and athenahealth 6.9%.
The result: most large health systems operate multiple EHR systems simultaneously. A Becker's Hospital Review report notes the average health system uses 18 different EHR vendors across affiliated providers, each with proprietary data formats and protocols that require custom integration work. KLAS research confirms the impact: only 44% of clinicians agree their EHR provides expected integration with outside organizations, and 47% cannot quickly find important patient information from external sources.
HIPAA and Security Compliance
Every integration point is a potential liability. In 2024, HHS OCR recorded 663 large healthcare data breaches affecting approximately 242.9 million people, with hacking and IT incidents accounting for 81% of those breaches.
IBM's 2025 Cost of a Data Breach Report identifies healthcare as the highest-cost industry, at an average of $7.42 million per breach. HIPAA-compliant architecture is the baseline requirement, not a differentiator. That means every integration must include:
- Encrypted data transmission
- Audited access controls
- Business Associate Agreements at each integration point
The Patient Identification Problem
The U.S. has no national patient identifier. Without one, systems matching records across organizations rely on demographic matching (name, date of birth, address), and it fails more often than most people realize. Pew research found patient match rates can drop to 50% across organizations, with 1 in 5 hospital CIOs reporting patient harm from record mismatches in the prior year.
For time-sensitive workflows like transport coordination, a mismatched record isn't just an administrative error. It's a patient safety event.
Operational and Cost Complexity
Technical barriers are only part of the picture. Integration projects also carry significant organizational weight:
- Hospital IT security reviews and approval processes can extend timelines by months
- High vendor fees and lack of realistic clinical testing data are cited as top barriers by 47–50% of digital health companies
- Staff adoption often determines whether an integration succeeds or gets abandoned; even technically sound integrations fail when clinical staff default to manual workarounds
The "build vs. buy" decision compounds this: building custom integrations requires sustained engineering resources and ongoing maintenance. Purpose-built platforms with existing EHR certifications can cut deployment timelines from months to weeks.
EHR Integration in Patient Logistics and Care Coordination
Patient logistics — transport, care transitions, home health ordering, DME coordination — is one of the most friction-heavy areas in healthcare operations, and one of the least integrated with the EHR.
Transportation barriers delay or prevent care for an estimated 3.6 million people annually and account for at least 25% of missed clinic appointments. Delayed discharges compound the problem, with research citing lack of information sharing and inefficient capacity coordination as primary drivers of prolonged length of stay.
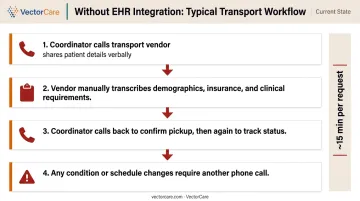
When transport systems are disconnected from the EHR, the typical workflow looks like this:
- Coordinator calls transport vendor with patient details verbally
- Vendor manually transcribes demographics, insurance, and clinical requirements
- Coordinator calls back to confirm, then again to track status
- Any changes to the patient's condition or pickup time require another phone call
Phone calls dominate: 87% of healthcare professionals report using them as their primary care coordination channel, with fax still used by 27%.
What Integration Changes
EHR-integrated logistics platforms eliminate that loop. Patient demographics, clinical conditions, insurance coverage, and care requirements pull automatically from the EHR into the transport or service request. The coordinator initiates the request from within the clinical workflow; the vendor receives a complete, structured order without a phone call.
The operational difference is measurable. Internal benchmarks from VectorCare's platform show what that shift looks like in practice:
- Coordination time per request: ~15 minutes → under 2 minutes
- Provider response time: 35+ minutes → ~40 seconds
- Primary coordination method eliminated: phone calls replaced by structured, EHR-sourced orders
VectorCare's SoFaaS Platform
Those gains depend on integration being achievable in the first place — and for most logistics vendors, the EHR connectivity barrier is the bottleneck. VectorCare's forthcoming SoFaaS (SMART on FHIR as a Service) platform, launching in 2026, is built to close that gap. Rather than treating EHR connectivity as a months-long IT project, SoFaaS enables healthcare vendors and logistics providers to build and deploy EHR-embedded applications in weeks — then scale without large internal development teams.
For hospitals and logistics providers that have deferred integration because of cost or complexity, that distinction matters. It moves EHR connectivity from a capital project into an operational decision.
EHR Integration Best Practices for Healthcare Organizations
Map Workflows Before Evaluating Vendors
The most common integration failure isn't technical — it's misalignment between the system and the actual workflow it's supposed to support. Before evaluating standards or platforms, map the specific clinical and operational touchpoints where data gaps cause the most friction.
Integration that fits naturally into existing workflows gets used. Integration that forces workarounds gets abandoned.
Require Standards Compliance, Not Just "Integration"
"We integrate with Epic" covers a wide range of actual capabilities. Push vendors to be specific:
- HL7 v2 — Are ADT messages, lab orders, and billing feeds supported?
- FHIR R4 — Is this production-grade or a sandbox connection?
- SMART on FHIR — Is the app listed on Epic Showroom or equivalent?
- Security certifications — HIPAA, SOC 2 Type II, and any relevant state requirements
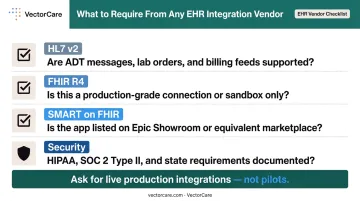
Ask for documentation of live, production integrations — not pilots. Standards-based integrations are more portable, easier to maintain, and better positioned for evolving federal requirements than proprietary connections.
Measure Outcomes, Not Just Connectivity
Technical connectivity is a starting point, not a result. Track metrics that reflect actual operational impact:
- Reduction in manual coordination tasks per transport or referral
- Decrease in communication-related delays at discharge
- On-time performance improvement for patient transfers
- Length of stay trends for patients routed through integrated workflows
VectorCare tracks these outcomes across its hospital partners, and the pattern holds: the gap between "technically connected" and "meaningfully integrated" closes only when workflow alignment and adoption are measured alongside the technical deployment. That measurement discipline is what separates integrations that stick from ones that quietly get routed around.
Frequently Asked Questions
What is an EHR integration?
EHR integration is the process of connecting an electronic health record system to other healthcare software or platforms so patient data flows automatically between them. It eliminates manual data entry and enables connected workflows across care settings without requiring staff to re-enter information in multiple systems.
What are the EHR integration standards?
The three primary standards are HL7 v2 (legacy message-based hospital workflows), FHIR R4 (modern REST API for web and mobile apps), and SMART on FHIR (secure EHR-embedded app framework). U.S. federal regulations mandate FHIR API support under 45 CFR 170.215.
What is the difference between HL7 and FHIR?
HL7 v2 is a message-based standard used for decades in hospital operational workflows — lab orders, ADT events, billing feeds. FHIR is a modern API-based standard designed for web and mobile health applications using REST and JSON. Most healthcare environments require both: HL7 v2 keeps legacy systems running while FHIR powers newer digital health layers.
What is SMART on FHIR?
SMART on FHIR is a standardized framework that allows third-party applications to launch securely from within an EHR, pre-populated with patient context and authenticated through standardized security protocols. Clinicians access external tools without leaving their workflow. It is now widely supported by major EHR platforms, most notably Epic.
What are the biggest challenges in EHR integration?
Three challenges dominate: vendor fragmentation requiring custom work per EHR system, HIPAA compliance at every integration point (breach costs average $7.42M), and operational complexity from hospital security reviews and staff adoption barriers.
How does EHR integration improve patient care coordination?
Integrated EHRs eliminate manual handoffs — phone calls, faxes, duplicate data entry — that delay care transitions and post-acute service initiation. Care teams work from complete, real-time records rather than fragmented data, reducing the communication gaps that extend length of stay and increase transition errors.