The numbers reflect the stakes. Average hospital length of stay rose 19.2% in 2022 versus 2019, with delays for patients awaiting post-acute discharge rising nearly 24%. Meanwhile, a 2024 CDC-published meta-analysis found that outpatient follow-up within 30 days was associated with a 21% lower all-cause readmission risk — a figure that goes directly to how well logistics is managed after discharge.
This article covers what patient logistics actually is, why it has become a strategic and clinical priority, what the real costs of doing it poorly look like, and how modern technology is reshaping the field.
Key Takeaways
- Patient logistics is the full coordination layer connecting transport, discharge planning, home health, DME, and post-acute care — not just scheduling rides
- Fragmented logistics causes delayed discharges, missed follow-ups, and avoidable readmissions that cost hospitals millions annually
- Value-based care has converted logistics failures into direct financial penalties
- Modern platforms with EHR integration and automated dispatching can reduce coordination time by 90% or more
- Treating logistics as infrastructure — not administration — is what separates high-performing health systems from struggling ones
What Is Patient Logistics in Healthcare?
Patient logistics is the coordinated management of all non-clinical services that move patients through the healthcare continuum. This includes transport, discharge coordination, home health scheduling, DME delivery, and post-acute care placement.
It is distinct from clinical care, but inseparable from clinical outcomes.
Transport vs. Logistics: A Critical Distinction
Patient transport is one service. Patient logistics is the orchestration layer that connects every stakeholder involved in a care transition:
- Hospitals and health systems manage bed availability and discharge throughput
- Case managers and discharge planners coordinate services across multiple vendors simultaneously
- Ambulance and NEMT providers fulfill transport requests at varying acuity levels
- Home health agencies schedule post-discharge visits
- DME suppliers deliver equipment to patients' homes before or at discharge
- Payers authorize and fund care transitions
- SNFs and post-acute facilities accept and onboard incoming patients
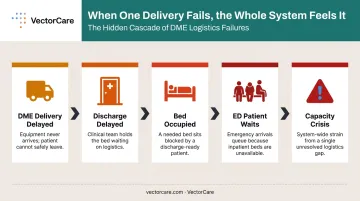
Each stakeholder's actions affect every other. When a DME delivery is delayed, a patient's discharge is delayed. When discharge is delayed, a bed is occupied. When a bed is occupied, an ED patient waits. The chain reaction from a single logistics failure ripples across the entire system.
Patient logistics is foundational healthcare infrastructure — not a scheduling problem, not a back-office function. When it's treated as either, the consequences surface in avoidable readmissions, declining quality scores, and margins that erode faster than anyone can explain.
Why Patient Logistics Has Become a Strategic Priority
The demand pressure on patient logistics is growing from multiple directions at once.
Demographic and Disease Burden
The US population aged 65 and older reached 55.8 million in 2020, up 38.6% from 2010. Globally, WHO projects that 1 in 6 people will be age 60 or older by 2030. Older adults generate much higher logistics complexity — requiring transport, post-acute placement, DME, and home health at far higher rates than younger populations.
Chronic disease amplifies this further. 76.4% of US adults — 194 million people — had at least one chronic condition in 2023, including 93% of older adults. Patients managing multiple chronic conditions cycle repeatedly through the care continuum, generating ongoing logistics needs that manual coordination simply cannot scale to meet.
Value-Based Care Has Changed the Stakes
Fee-for-service treated a delayed discharge as an administrative frustration. Value-based contracts price that same failure as a readmission penalty, a reduced reimbursement, and a lower quality score — with real dollar consequences on the balance sheet.
HCP-LAN's 2024 APM Measurement Report shows how far that shift has already gone:
| Metric | Figure |
|---|---|
| Aggregate payments in APM Categories 3–4 | 45.2% |
| Payments in downside-risk arrangements | 28.5% |
| Traditional Medicare payments in Categories 3–4 | 42% |
| Traditional Medicare in downside-risk categories | 33.7% |
| Hospitals facing HRRP penalties ≥1% (FY 2026) | 8.1% (up from 7% in FY 2025) |
CMS caps HRRP payment reductions at 3% — but even a 1% penalty on a large health system represents millions in lost reimbursement. For CFOs and CMOs, logistics failures are no longer an operational footnote; they're a line item.
Workforce Pressure Compounds the Problem
Financial exposure from value-based penalties lands hardest on teams that are already stretched thin. Nurses and case managers operating under high cognitive load absorb manual logistics coordination on top of clinical work — sequential calls to transport vendors, fax-based DME orders, individual calls to SNF admissions teams — all tasks that pull attention away from patients.
VectorCare's own data shows a single patient discharge can require 5–10 phone calls across multiple vendors, each averaging 8–12 minutes. The math compounds quickly:
- A hospital managing 30 discharges per day at 5 calls each (8 min/call) = ~200 staff hours per month
- At 50 discharges per day with 10 calls each (12 min/call) = ~1,000 staff hours per month
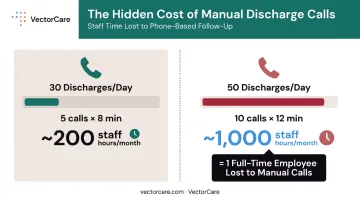
At the higher end, that's the equivalent of a full-time employee doing nothing but making phone calls — every month, every year.
The Hidden Costs of Fragmented Patient Logistics
Most logistics failures are not caused by a shortage of providers or services. They are caused by fragmented communication across siloed systems — fax, phone, and separate software platforms that leave no single stakeholder with a complete picture of where a patient stands in their transition.
Bed-Day Costs
KFF's AHA-based data shows hospital expenses per adjusted inpatient day run approximately $3,297 in the US. Every day a patient occupies a bed because discharge logistics weren't ready is a day of capacity consumed and revenue unrealized. A 2024 peer-reviewed analysis found that delayed discharges are associated with a 30.7% increase in daily expenses — a compounding effect that makes logistics delays far more expensive than they appear on the surface.
Readmission Risk from Missed Follow-Up
The CDC meta-analysis cited earlier is direct: completing outpatient follow-up within 30 days is associated with a 21% reduction in all-cause readmission risk, with even stronger effects for heart failure (27%) and stroke (24%). Transportation barriers are among the leading non-clinical reasons patients miss those appointments.
Those missed appointments carry a direct price tag:
- 3.8 million US hospital readmissions occurred in 2018
- Average cost per readmission: $15,200
- Heart failure readmissions alone: $3.49 billion annually
When logistics failures drive preventable readmissions, that cost is measurable and attributable.
The Root Cause: Communication Breakdown
ONC's 2023 data found that hospitals exchange health information electronically with external hospitals and ambulatory providers far more often than with long-term and post-acute care providers — precisely where most discharge coordination happens. That interoperability gap means care teams are still relying on phone and fax to coordinate the most complex patient transitions.
That reliance on manual communication doesn't just slow things down — it creates downstream failures across the board:
- Credential verification lapses on unverified transport vendors
- Documentation gaps that expose facilities during regulatory audits
- Liability risk when patient handoffs happen outside any auditable system
Each of these failures is traceable back to the same root: no single platform connecting all the stakeholders in a patient's transition.
Core Components of a Modern Patient Logistics System
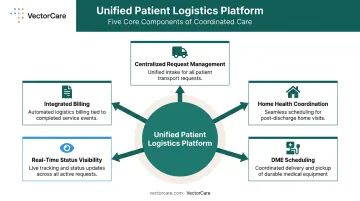
Patient logistics is not one problem. It is a set of interconnected problems — transport, discharge, equipment, billing, compliance — that break down when managed in isolation. A unified platform addresses all of them at once.
A unified patient logistics platform must cover:
- Centralized request management — handling all transport types (ALS, BLS, gurney van, rideshare, air medical) from a single interface
- Home health coordination — scheduling visits alongside discharge, not after
- DME scheduling — ensuring equipment arrives before or at the time of discharge
- Real-time status visibility — accessible to every stakeholder, not just the requester
- Integrated billing — eliminating the reconciliation burden of managing multiple vendor invoices separately
Credentialed Provider Networks
A modern platform must include a vetted marketplace of transport and service vendors with automated credential verification. Hospitals should not be manually checking whether every dispatched provider is compliant — that verification should happen in the background, every time, automatically.
EHR Integration Is Not Optional
With over 99% of US non-federal acute care hospitals having adopted certified EHR technology, and Epic continuing to expand its market share, patient logistics must connect to the clinical record. Demographic data, insurance information, and discharge orders need to flow automatically into logistics requests. The operational benefits are direct:
- Eliminates duplicate data entry across clinical and logistics teams
- Reduces transcription errors that delay or misdirect transport requests
- Keeps clinical and operational staff working from the same information in real time
How Technology and Automation Are Transforming Patient Logistics
Automated Dispatching Intelligence
Traditional transport scheduling relied on sequential phone calls — contact one provider, wait for a response, call the next if unavailable. Automated dispatching flips that model entirely. A single broadcast reaches an entire network of credentialed providers simultaneously, with the system selecting the appropriate match based on policy-driven rules.
VectorCare's Automated Dispatching Intelligence (A.D.I.) operates at the infrastructure level: it processes a new request every 23 seconds and sending broadcasts every 12 seconds across its network. In 2025, A.D.I. saved healthcare systems and suppliers more than 100,000 hours by eliminating the manual back-and-forth that previously defined transport coordination.
SMART on FHIR: Logistics Inside the Clinical Workflow
The SMART App Launch standard, as defined by HL7, allows third-party applications to connect to EHR data and launch from inside the EHR environment. For patient logistics, this architecture is significant: it means a case manager can initiate a transport request, schedule a home health visit, and order DME from inside Epic — without switching systems or re-entering patient data.
VectorCare's SMART on FHIR Epic integration does exactly this. Patient demographics, insurance information, and clinical context pull automatically from the record. Every logistics event writes back to the chart. One large health system reduced scheduling time from 31 minutes to under one minute using this embedded workflow.
AI Agents and Autonomous Coordination
Embedded workflows eliminate the need to switch systems — but AI agents take coordination a step further by removing manual review from routine decisions entirely. VectorCare's platform handles the full response cycle autonomously:
- Processes 1 to 1,000 provider responses returned from a single broadcast
- Selects the best match based on pre-defined policy and bidding logic, instantly
- Manages follow-up confirmations without coordinator intervention
- Escalates exceptions to human review only when needed
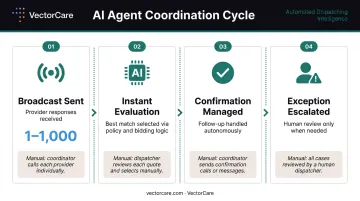
Without this, a coordinator would manually evaluate each response — one by one.
Real-Time Visibility and Analytics
A platform that provides live tracking of transport status, discharge timelines, and vendor performance lets administrators intervene before delays cascade into missed appointments or extended stays. When a transport is delayed, the care team knows immediately — not when a patient fails to show up for a follow-up appointment a week later.
VectorCare's platform generated 2.3 million broadcasts in 2024 with contract value exceeding $570 million, across a network spanning more than 2,500 healthcare facilities.
Its no-code workflow builder lets care teams design and modify logistics workflows without IT resources. The SMART on FHIR infrastructure now extends through SoFaaS (SMART on FHIR as a Service), enabling other healthcare vendors to embed their own services inside EHR workflows without building the compliance and integration stack from scratch.
Measuring the ROI of Better Patient Logistics
Operational Efficiency
Orange County Health Care Agency's implementation of VectorCare's platform reduced average transport coordination time from 45 minutes to 4.5 minutes per request — a 10x reduction. For a hospital managing dozens of discharges daily, this scale of time savings translates directly into staff hours recovered and redirected toward patient care.
VectorCare's broader data shows that a 250-bed facility can reduce annual scheduling hours from approximately 4,700 to under 500 — labor savings that compound across years.
Those efficiency gains translate directly to the bottom line.
Financial Outcomes
VectorCare has documented over $500,000 in average annual savings per hospital partner, driven by reduced bed days, lower staff hours spent on coordination, and fewer readmissions attributable to logistics failures. One large California payer-provider using A.D.I. for automated transport vendor selection saved $22 million annually while eliminating over 10,000 staff hours in manual coordination.
Clinical Quality and Patient Experience
The connection between logistics performance and clinical quality metrics is direct:
- Shorter discharge-to-transport times reduce deconditioning and infection exposure during unnecessary hospital stays
- Coordinated post-acute placement reduces complication rates in the weeks following discharge
- Reliable transportation to follow-up appointments reduces 30-day readmission rates across multiple diagnosis categories
For health systems operating under value-based care contracts, these outcomes directly affect quality scores, reimbursement rates, and total cost of care — making logistics performance a measurable factor in financial sustainability.
Frequently Asked Questions
What is patient logistics in healthcare?
Patient logistics is the full coordination layer covering transport, discharge planning, home health scheduling, DME delivery, and post-acute care placement. It is distinct from patient transport, which is one service within that broader infrastructure.
How does poor patient logistics affect hospital operations?
Fragmented logistics causes delayed discharges, prolonged bed occupancy, missed follow-up appointments, and increased readmission risk — all of which carry direct financial consequences under value-based care contracts.
What is the difference between patient transport and patient logistics?
Transport is one service within patient logistics. The broader distinction matters operationally: patient logistics connects every care transition service — home health, DME, post-acute placement, and payer coordination — into a single infrastructure, while transport is simply one node within it. Treating them as interchangeable is what leads to fragmented coordination and delayed discharges.
How does technology improve patient logistics coordination?
Automation, EHR integration, real-time tracking, and AI dispatching eliminate manual steps and reduce communication delays. The result is a unified view of patient status for all stakeholders, with no need to manage multiple systems or make sequential phone calls.
What role does AI play in patient logistics?
AI handles automated dispatching, vendor selection, scheduling optimization, and response processing. It evaluates provider responses in split seconds, selecting the most appropriate match based on policy-driven rules without requiring human review of each option.
How can hospitals reduce discharge delays through better logistics?
Four changes move the needle fastest:
- Automate transport scheduling to eliminate manual phone coordination
- Integrate logistics into the EHR so case managers never leave the clinical record
- Coordinate home health and DME simultaneously, not sequentially
- Use real-time status tracking to catch delays before they cascade