Introduction
Picture a typical Tuesday morning in a 300-bed hospital: beds occupied by patients cleared for discharge hours ago, transport coordinators working through a phone queue that never empties, and nurses hunting down status updates that no one system can provide. This isn't a staffing problem. It's a logistics infrastructure problem.
The financial consequences are concrete. When discharge logistics fail, a Level I trauma center study found the average delay ran 6 days — generating $715,403 in annual excess bed costs at a single facility. Each hour of ambulance diversion is associated with $1,086 in forgone hospital revenue, according to a peer-reviewed Annals of Emergency Medicine study.
The upside of getting this right is equally measurable. A 2024 BMJ Open Quality study of the SAFER patient-flow bundle found median hospital length of stay dropped from 19.3 days to 14.1 days, with discharges rising 21%.
Those results don't happen by accident. The sections below break down the strategies that drive them: predictive bed management, early discharge planning, centralized transport coordination, structured inter-facility transfer protocols, and the technology infrastructure that ties them together.
Key Takeaways
- Patient flow logistics is an infrastructure problem, not a scheduling problem—reactive fixes create new bottlenecks
- Discharge planning must begin at admission, not the morning a patient is medically cleared
- Centralized transport coordination reduces duplication and creates accountability across every handoff
- EHR adoption is near-universal — real-time coordination integration is not
- Cross-unit metrics reveal flow problems that departmental numbers hide
What Is Patient Flow Logistics—and Why Does It Matter?
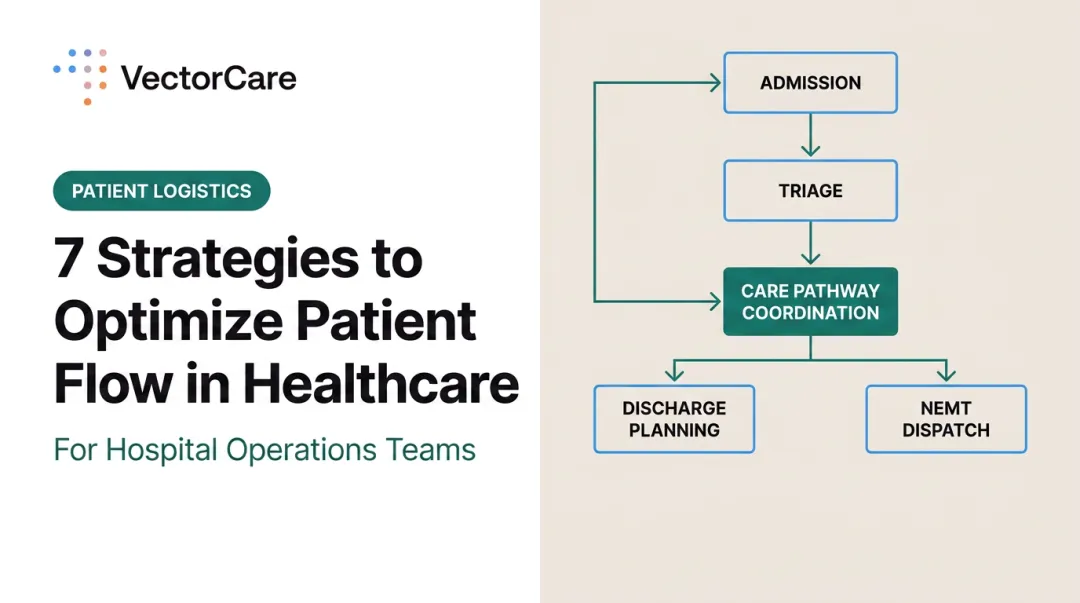
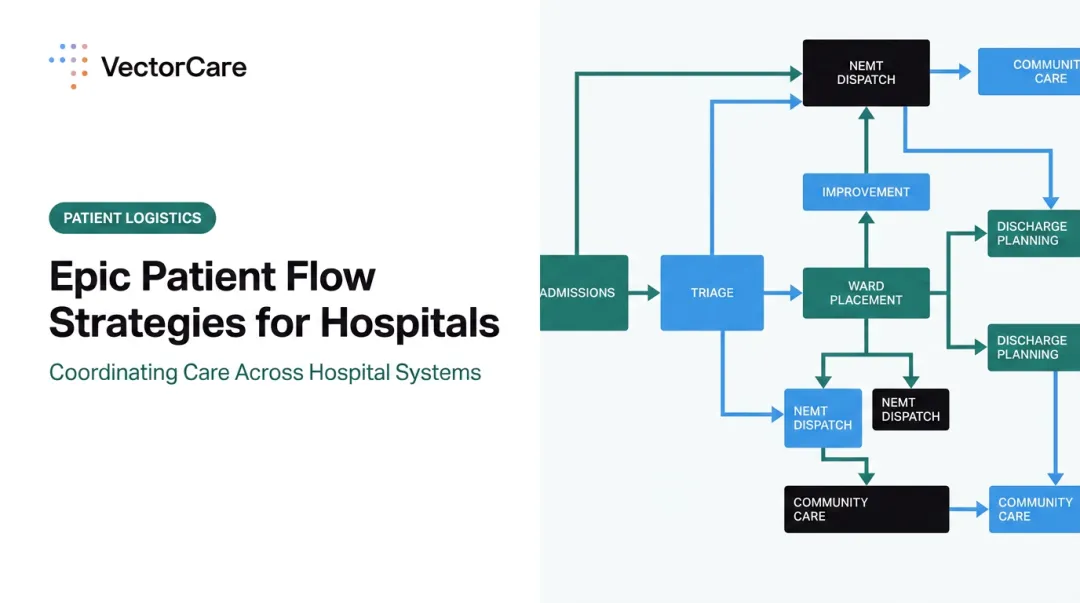
Patient flow logistics is the coordinated management of every movement a patient makes across the care continuum: initial transport requests, bed assignments, intra-facility transfers, discharge, and post-acute follow-up. It encompasses the resources that support those movements — staff, vehicles, equipment, and information systems.
The distinction between treating this as a scheduling problem versus an infrastructure problem is where most hospitals get stuck.
Treat it as a scheduling problem, and fixes stay reactive and siloed. A unit manager addresses the transport backlog. A case manager expedites one discharge. A coordinator makes more calls. Each fix is local; none of them change the underlying system.
Treat it as infrastructure, and coordination becomes predictive and cross-functional. Bed assignments anticipate discharge timing, transport requests trigger automatically, and environmental services receive alerts without manual follow-up. The system moves patients forward rather than waiting for someone to push.
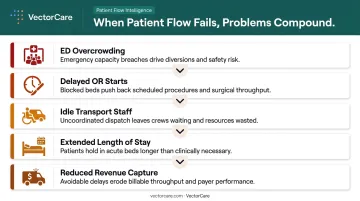
The downstream consequences of unoptimized flow compound one another:
- ED overcrowding as admitted patients wait for inpatient beds
- Delayed OR starts when post-surgical beds aren't cleared
- Idle transport staff because requests arrive unevenly and unpredictably
- Extended length of stay from discharge logistics that begin too late
- Reduced revenue capture from diverted ambulances and slow transfer acceptance
None of these problems exist in isolation. Fix one poorly and another worsens — which is precisely why patient flow requires systems-level thinking, not just better task management.
Where Patient Flow Breaks Down: Common Bottlenecks
Most patient flow delays share the same root causes, even across facilities of different sizes and acuity levels.
The Manual Coordination Problem
Phone-based and fax-based transport requests remain common. When a nurse calls a transport coordinator, who calls a dispatcher, who calls back with a status update, cycle time expands at every step.
A 2018 time-motion study of 79 nursing shifts found that nurses spent roughly 10% of their time on delegable or non-nursing activities, with interprofessional communication consuming nearly 27 minutes per four-hour observation block — time pulled directly from patient care.
Discharge planning that begins on the day of discharge compounds the problem. When transportation scheduling, home health authorizations, and DME orders are initiated at the last minute, patients who are medically ready to leave sit in beds that other patients need.
The Data Silo Problem
Manual workarounds persist in part because the underlying systems don't communicate. Despite over 99% of U.S. non-federal acute-care hospitals having certified EHRs as of 2024, only 43% routinely engaged in all four domains of interoperable exchange as of 2023.
Only 42% reported that clinicians routinely used outside electronic information at the point of care.
When EHR systems, bed management platforms, and transport dispatch tools don't share real-time data, coordinators work from incomplete information. They call to verify status the system should already know. They re-enter patient data that already exists in the record.
Only 16% of hospitals sent summary-of-care records to most or all long-term and post-acute care providers — which explains why so many patients arrive at skilled nursing facilities without the documentation needed to begin care.
Core Strategies for Optimizing Patient Flow Logistics
Implement Predictive Bed Management
Reactive bed assignment—responding to a discharge after it happens—guarantees delays. A just-in-time model uses historical admission patterns, real-time census data, and anticipated discharges to get ahead of capacity constraints.
The key mechanism is automatic downstream triggering. When a discharge is confirmed, bed cleaning should initiate simultaneously, not after a separate manual request. Environmental services receives the alert. The next patient assignment is queued. That collapse in cycle time—eliminating the gap between one task completing and the next beginning—is where predictive bed management delivers its value.
This requires systems that talk to each other without human intermediaries. A bed management platform that can't notify environmental services, or an EHR that can't surface discharge status to a transport coordinator, forces staff back into the phone queue.
Start Discharge Planning at Admission
CMS discharge-planning regulations require hospitals to identify high-risk patients at admission—or shortly after—and complete evaluations before discharge delays occur.
The regulatory standard reflects a simple operational reality: discharge logistics take time. That clock needs to start before a patient is medically cleared to leave.
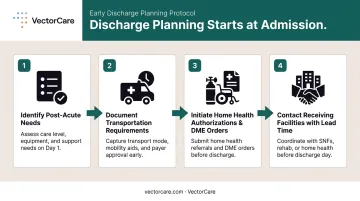
In practice, "discharge planning begins at admission" means:
- Case managers identify post-acute placement needs on day one
- Transportation requirements are documented early, not scheduled the morning of discharge
- Home health authorizations and DME orders are initiated while the patient is still being treated
- Receiving facilities are contacted with enough lead time to prepare
A Cochrane review of 33 trials found that individualized discharge planning reduces initial hospital length of stay by 0.73 days in older medical patients and reduces unscheduled readmissions by about 11%. The AHA reported average hospital LOS increased approximately 19% in 2022 versus 2019—with a nearly 24% increase for patients discharged to post-acute care providers—underscoring how much is at stake when discharge planning lags.
Centralize Transport Coordination
Decentralized, unit-level transport requests create duplication, uneven workloads, and no system-wide visibility. Centralizing coordination—whether through a dedicated hub or an intelligent platform—changes the operating model.
A centralized model:
- Consolidates all requests into a single channel, eliminating competing unit-level queues
- Prioritizes by clinical urgency and timing, not by who called first
- Dispatches based on transporter availability and patient acuity across the full facility
- Logs every transport event—intra-facility and external—for accountability and analysis
- Covers all modalities: NEMT, ambulance, air medical, and intra-hospital transport
The operational benefit is transporter utilization. When requests arrive through a unified system, dispatchers see the full picture. Transporters aren't idle while one unit has a backlog and another has excess capacity.
Build Structured Inter-Facility Transfer Protocols
A 2018 study of a Level I pediatric trauma center found that mean time from transfer acceptance to admission was 202.7 minutes—with 56% of that elapsed time occurring before the patient even left the referring facility. That's not a transport problem. It's a coordination problem.
Structured protocols address this by establishing:
- Standardized clinical criteria for acceptance decisions
- Defined response time windows for receiving facility acknowledgment
- Automated notification workflows that eliminate sequential phone calls
- Clear handoff documentation exchanged digitally rather than verbally
Patient leakage—cases redirected to competing facilities because a transfer center didn't respond quickly enough—is a revenue loss that rarely appears on any report. Tightening response time windows and eliminating phone-tag handoffs keeps referring providers from looking elsewhere.
Leveraging Technology and Automation to Streamline Logistics
EHR Integration: Closing the Adoption-Integration Gap
High EHR adoption didn't automatically produce connected logistics systems. Most hospitals have the data they need sitting in a certified EHR—but that data doesn't flow in real time to transport dispatchers, bed management teams, or receiving facilities.
When scheduling, bed management, and transport systems pull from the same live data source, coordinators stop making verification calls. Patient information populates automatically. Status updates flow without manual follow-up. The coordination burden shifts from human labor to system infrastructure.
VectorCare's SMART on FHIR integration with Epic demonstrates this in practice. When a coordinator submits a transfer request through the platform, it automatically extracts patient data already documented in Epic and simultaneously broadcasts the request to available providers.
What previously consumed 35 minutes of sequential phone calls, one provider at a time, dropped to approximately 90 seconds in documented deployments. In one case, nine providers responded within forty seconds.
AI-Driven Dispatch and Real-Time Visibility
Machine learning models trained on historical transport data can forecast demand surges and recommend optimal routing before delays materialize. A 2024 peer-reviewed study from Taichung Veterans General Hospital validated real-time tracking and data-driven dispatch as a viable model for intra-hospital patient transport automation.
Real-time visibility dashboards—accessible simultaneously across nursing, transport, bed management, and environmental services—replace the manual follow-up call as the primary status-check mechanism. Automated alerts create accountability at each handoff point without requiring anyone to pick up a phone.
VectorCare's Automated Dispatching Intelligence (A.D.I.) puts this model into practice at scale. Key results across its customer base:
- Processes a new transport request every 23 seconds
- Saved healthcare systems more than 100,000 hours of administrative time in 2025
- 90% reduction in manual coordination tasks
- 45% decrease in communication-related delays
- Orange County Health Care Agency cut request processing time from 45 minutes to 4.5 minutes

The platform now serves over 2,500 healthcare facilities nationwide.
The Hybrid Human-AI Model
Full automation isn't the goal. Automation handles high-volume, rule-based coordination: routine scheduling, broadcast dispatching, status notifications. Clinical judgment stays with staff for exception handling, complex transfer scenarios, and decisions that require relationship context.
This balance produces more durable results than either extreme. Staff who understand how the system works are more likely to maintain it correctly — and staff who feel sidelined by it will find workarounds that erode the gains automation was meant to deliver.
Change Management: Getting Staff and Stakeholders Aligned
Most logistics optimization projects fail organizationally before they fail technically. Frontline staff who weren't consulted during implementation find workarounds. Clinical teams that distrust new workflows default to phone calls. The system gets bypassed, metrics don't improve, and the project loses organizational support.
Securing buy-in before system selection is the prerequisite most organizations skip. Nursing, transport, case management, and IT need to be at the table before a platform is chosen—not handed a training manual after the fact.
Practical alignment strategies:
- Designate a logistics champion — a clinician-adjacent leader who translates operational logic into clinical language and surfaces frontline concerns before they become adoption barriers
- Pilot on a single high-impact process (bed assignment or discharge coordination) and share results broadly before system-wide rollout
- Watch for the local optimization trap: a department that improves its own throughput metrics can create bottlenecks downstream. Cross-functional reviews tracking system-wide flow prevent this
VectorCare's SMART on FHIR architecture reduces one common adoption barrier by embedding logistics workflows directly inside Epic, so care teams don't have to learn a separate system.
That integration proved critical during wildfire evacuations at Kaiser Permanente. Their Regional Continuum of Care Administrator put it plainly: "I can't imagine that the team could have handled this sudden volume, and track where every patient was taken, as gracefully and calmly as they did, if they were still doing things the old way without VectorCare."
Key Metrics to Track and Measure Patient Flow Performance
Measuring performance without a baseline produces anecdotes, not evidence. Establish baseline figures for each metric before any optimization initiative begins.
Core operational metrics:
| Metric | What It Measures |
|---|---|
| Patient wait time (request to transport arrival) | Transport responsiveness |
| Bed turnaround time (discharge to next admission) | Environmental services coordination |
| Transfer acceptance time | Inter-facility handoff efficiency |
| Length of stay by unit and acuity | Overall flow performance |
| On-time transport performance rate | Transport reliability |
| Diversion hours | Capacity and access |
Measuring only departmental metrics creates structural blind spots. A transport department that hits its response time targets while the ED remains boarded is optimizing the wrong metric. Flow metrics need to cross unit boundaries to mean anything.
Operational improvements only make the case for sustained investment when tied to financial outcomes. Metrics worth tracking include:
- Revenue recovered from reduced diversion hours ($1,086 per diverted ambulance hour, per peer-reviewed data)
- Administrative labor cost reduction from automation
- Retained patient volume from faster transfer acceptance
- Avoided bed-day costs from shortened length of stay
VectorCare's average hospital partner reports over $500,000 in annual savings—primarily from reduced scheduling labor and bed throughput improvements. For a 250-bed hospital running 25 daily transports, cutting scheduling time from 31 minutes to under 3 minutes translates to roughly 4,300 hours per year freed from scheduling and coordination work.

Frequently Asked Questions
What does patient logistics mean?
Patient logistics is the coordinated management of patient movements across the care continuum—transport, bed assignment, transfers, and discharge—along with the staff, equipment, and systems that support them. It is an infrastructure function, not a scheduling task.
What does a patient flow team do?
A patient flow team oversees patient movement through a healthcare facility or system, managing bed assignments, transport requests, discharge coordination, and inter-facility transfers. Their goal is to minimize delays, reduce length of stay, and optimize capacity across units simultaneously.
What are the most effective strategies to improve patient flow?
The five highest-impact strategies are predictive bed management, discharge planning that starts at admission, centralized transport coordination, structured inter-facility transfer protocols, and technology integration that connects EHR, transport, and bed management systems in real time.
How does technology help optimize patient flow logistics?
Logistics platforms with EHR integration, AI-driven dispatch, and real-time visibility dashboards eliminate manual handoffs and reduce communication delays. Coordinators get a complete picture of patient status and transport availability, replacing phone queues with automated workflows.
What metrics should hospitals track to measure patient flow performance?
Track patient wait time, bed turnaround time, transfer acceptance time, length of stay, on-time transport performance rate, and diversion hours—measured cross-unit rather than by department to avoid creating blind spots where bottlenecks shift rather than resolve.
How long does it take to see results from patient flow optimization?
Pilot programs focused on a single high-impact process—such as bed assignment or discharge coordination—often show measurable improvements within weeks. System-wide gains in length of stay and leakage reduction typically emerge over three to six months with sustained change management effort.