Introduction
Healthcare organizations are under pressure from three directions simultaneously: patient volumes climbing, care coordination growing more complex across settings, and federal mandates requiring data sharing that legacy infrastructure wasn't built to support.
APIs — Application Programming Interfaces — have become the operational response to all three. Not as a trend, but as functional infrastructure with direct consequences: a discharge that takes hours instead of days, a prior authorization resolved in minutes rather than weeks, care teams working from complete patient records instead of information pieced together from phone calls.
The real value isn't abstract. According to CAQH's 2023 Index Report, US healthcare spent $82.7 billion on medical administrative transactions in 2023 — with $16.4 billion in identified savings opportunity from fuller electronic adoption. Much of that waste traces directly to manual processes that APIs can replace.
This article explains what healthcare APIs actually do, the three advantages that matter most operationally, and what it costs organizations that still rely on phone calls, faxes, and manual re-entry.
Key Takeaways
- Healthcare APIs let different systems — EHRs, payers, transport platforms, labs — exchange data automatically without manual re-entry
- APIs drive three core gains in healthcare operations: real-time interoperability, workflow automation, and regulatory compliance
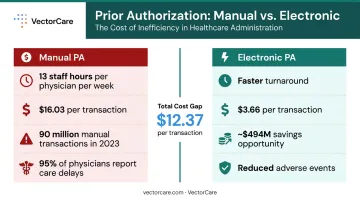
- In 2023, 90 million of 233 million prior authorization transactions were still manual — costing $16.03 each vs. $3.66 electronically
- CMS mandates FHIR R4-based APIs for regulated payers, with full compliance required by January 1, 2027
- Organizations that treat APIs as core infrastructure — rather than one-off IT projects — see compounding returns in cost, quality, and speed
What Is a Healthcare API?
A healthcare API is a standardized communication layer that lets two different software systems exchange data on demand — without a human in the middle. When a hospital's EHR queries a payer's system to verify coverage, or a transport platform pulls patient demographics automatically when a discharge coordinator opens a request, that's an API doing the work that phone calls and fax machines used to do.
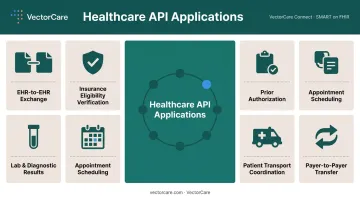
Where Healthcare APIs Are Applied
APIs show up across nearly every operational workflow in healthcare:
- EHR-to-EHR data exchange — sharing records across facilities and systems
- Insurance eligibility verification — real-time coverage confirmation at the point of care
- Prior authorization — automated submission and response between provider and payer systems
- Lab and diagnostic results — structured result delivery directly into clinical workflows
- Appointment scheduling — system-to-system booking without portal logins
- Patient transport coordination — connecting discharge orders to logistics platforms automatically
- Payer-to-Payer data transfer — moving member records when patients switch plans
The standard underlying most of these today is FHIR (Fast Healthcare Interoperability Resources), defined by HL7 as the common language for structured healthcare data exchange. By 2024, 70% of non-federal acute care hospitals had enabled patient access using FHIR-configured apps — up from 56% in 2021.
What that adoption rate reflects is practical demand: care teams need complete information at the moment a decision is made, not minutes later after a phone call or a fax gets processed.
Key Advantages of Healthcare APIs
Three advantages stand out for their direct, measurable impact on cost, care quality, speed, and compliance risk. Each builds on the others when APIs connect systems consistently rather than through isolated, one-off integrations.
Advantage 1: Real-Time Interoperability Across Fragmented Systems
Healthcare data is siloed — not by design, but by accident. A patient moving from an ED to a skilled nursing facility may have records spread across three EHRs, a transport system, a payer database, and a pharmacy. Without APIs, care teams reconcile those records manually at every handoff.
With APIs, a system pulls the data it needs automatically at the moment it's needed. Demographics, diagnoses, and insurance details flow to the right system without staff re-entering them from scratch.
Why fragmentation is a safety problem, not just an efficiency problem:
AHRQ cites landmark research showing nearly 20% of patients experienced adverse events within three weeks of discharge — a consequence, in large part, of incomplete information at care transitions. A JAMIA study found duplicate testing in 32% of examined transfer cases, with at least one non-clinically indicated test in 20% — waste that begins with data that didn't follow the patient.
Approximately 1.5 million patients are transferred between acute care hospitals in the US each year. At that volume, manual chart reconciliation at each handoff isn't a workaround — it's a structural risk.
KPIs this advantage influences:
- Length of stay
- Care transition error rates
- Duplicate test orders
- Time-to-transfer
- Staff hours spent on manual data reconciliation
Where this hits hardest: High-volume, multi-site environments — health systems managing dozens of facilities, transfer centers coordinating hundreds of daily patient movements. VectorCare's SMART on FHIR Epic integration illustrates this in practice: when a transport or service request is initiated, the platform automatically pulls patient demographics, height, weight, allergies, and vitals from Epic — eliminating the manual intake steps that previously required phone calls and created transcription errors. The integration writes data back to the medical record as well, making the exchange bidirectional.
Advantage 2: Workflow Automation That Reduces Administrative Burden
Prior authorization remains one of the clearest examples of where manual healthcare workflows break down at scale.
The AMA's 2025 Prior Authorization Physician Survey found that practices complete 39 prior authorizations per physician per week, consuming 13 hours of physician and staff time. 95% of physicians reported that PA delays care. 26% reported serious adverse events tied to those delays.
CAQH data puts the cost gap in plain terms: manual PA costs providers $16.03 per transaction versus $3.66 electronically — across 90 million manual PA transactions in 2023 alone. That's a savings opportunity of nearly $494 million from PA automation alone.
How APIs change this:
Once an API connection exists between two systems, a trigger in one system initiates actions in another — automatically. A discharge order generates a transport request. An eligibility verification kicks off before the patient reaches registration. A PA submission goes out the moment an order is placed, with a response returned without a single phone call.
VectorCare's platform demonstrates this in the air transport context: the scheduling workflow that previously required roughly 15 minutes of coordinator time — and approximately six phone calls to locate an available aircraft — drops to under two minutes through API-connected real-time availability and direct EHR integration.
KPIs this advantage influences:
- Authorization turnaround time
- Transport scheduling time
- Staff hours spent on administrative tasks
- Error rates from manual data entry
- Cost per transaction
When it matters most: Transfer centers handling hundreds of daily movements, NEMT coordinators managing dozens of concurrent requests, health systems processing thousands of prior authorizations monthly — at these volumes, each automated transaction multiplies the return.
Advantage 3: Regulatory Compliance and Standardized Data Access
Healthcare API adoption isn't optional for regulated payers — it's a legal requirement with enforcement consequences.
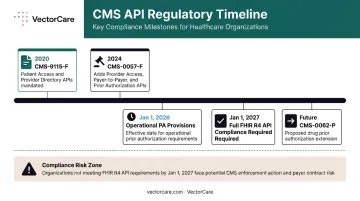
The 2020 CMS Interoperability and Patient Access Final Rule (CMS-9115-F) required Medicare Advantage organizations, Medicaid managed care plans, CHIP programs, and QHP issuers to implement Patient Access and Provider Directory APIs on FHIR standards. The 2024 CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) extended those requirements, adding Provider Access, Payer-to-Payer, and Prior Authorization APIs — all on HL7 FHIR R4 — with operational PA provisions effective January 1, 2026 and full API compliance required by January 1, 2027.
A proposed 2026 rule (CMS-0062-P) would extend similar requirements to drug prior authorization, suggesting the regulatory direction is toward broader, not narrower, API mandates.
What non-compliance looks like:
For MA organizations, CMS enforcement mechanisms include warning letters, corrective action plans, civil money penalties, and sanctions. For information blocking specifically, certified health IT developers, HIEs, and health information networks face civil monetary penalties of up to $1 million per violation under ONC's Cures Act Final Rule.
CMS estimated the 2024 rule would reduce provider burden by at least 220 million hours and $16 billion over 10 years, against implementation costs of approximately $1.6 billion. That ratio — roughly 10:1 — favors early adoption over emergency compliance.
What to measure:
- Compliance audit readiness
- Prior authorization turnaround time
- Cost of integration development
- Data sharing partner count
- Patient access to records
When it matters most: This is non-negotiable for Medicare Advantage organizations, Medicaid managed care plans, CHIP programs, and QHP issuers on federal exchanges. It also affects any health system or vendor building new digital products that must connect to regulated payer systems — the sooner FHIR-based API patterns are established, the cheaper future integrations become.
What Happens When Healthcare APIs Are Missing
The consequences of operating without API infrastructure are measurable, not theoretical. Four patterns show up consistently across facilities that lack it:
- Fragmented records increase clinical risk. When data doesn't move with the patient, care teams fill gaps with guesswork. That's the direct explanation behind 20% post-discharge adverse events and a 32% duplicate testing rate during transfers.
- Manual coordination consumes staff capacity. In 2023, 31% of prior authorization transactions were still fully manual — phone calls, faxes, portal logins. Each step is a potential error and a consumed staff hour that could be spent on patient care.
- Point-to-point workarounds don't scale. Every new care partner, transport vendor, or payer relationship added without an API layer requires custom integration work. The result is a growing web of one-off connections, each one a future maintenance liability.
- Regulatory deadlines are arriving without warning. Organizations that haven't moved toward FHIR-based API infrastructure face compounding costs as 2026 and 2027 deadlines approach: emergency development under time pressure plus potential penalties for non-compliance.
Taken together, these gaps push organizations into reactive mode: staff spend their time resolving data problems rather than coordinating care, and the cost of that friction scales directly with patient volume.
How to Get the Most Value from Healthcare APIs
APIs deliver the most value when treated as infrastructure, not installed as isolated integrations.
The distinction matters. Infrastructure thinking means every new system connection is built on the same standard — FHIR — so integrations are reusable and maintainable rather than rebuilt from scratch each time.
Platforms like VectorCare, built API-native with HIPAA-secure SMART on FHIR integration, function as a ready-made logistics infrastructure layer. Hospitals connect once rather than building separate integrations for transport, DME, home health, and payer verification independently.
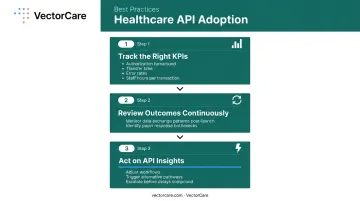
Three practices that separate high-performing organizations:
Track the KPIs APIs were meant to move : authorization turnaround, transfer initiation time, error rates, staff hours per transaction. If those numbers aren't improving, the integration isn't being used effectively.
Review outcomes continuously, not just at go-live — data exchange patterns reveal friction points that aren't visible before launch. A payer that consistently takes three days to respond to PA requests is a workflow problem, not just a data problem.
Treat API insights as signals to act on, not just report — when data reveals a bottleneck, high-performing teams adjust workflows, trigger alternative pathways, or escalate before delays compound.
Conclusion
Healthcare APIs solve a problem that coordination software alone can't: they make data portable, timely, and trustworthy across every handoff — from discharge planning to transport dispatch to post-acute follow-up. Care teams get the information they need when they need it, and manual errors that drive cost and patient harm stop propagating through the system.
Each integration built on a standard data layer — FHIR in particular — makes the next connection faster and cheaper. Organizations building on that foundation now aren't just solving today's coordination problems. They're creating infrastructure that holds as care models evolve, regulations update, and patient expectations rise. VectorCare's SMART on FHIR integration with Epic is one example of what that looks like in practice: patient data flows automatically into logistics workflows without manual re-entry, at every point of care.
The next interoperability mandate will come. Organizations with FHIR-based API infrastructure already running will adapt quickly. Those without it will spend months catching up — months during which care transitions, transport coordination, and discharge workflows continue running on manual effort and fragmented data.
Frequently Asked Questions
What does API stand for in healthcare?
API stands for Application Programming Interface — a standardized set of rules that allows two software systems to communicate and exchange data. In healthcare, APIs enable EHRs, payers, pharmacies, and logistics platforms to share patient information automatically, without manual re-entry at each handoff.
What is an example of an API in healthcare?
When a hospital discharge coordinator initiates a patient transport request and the transport platform automatically pulls demographics, vitals, and clinical data from the EHR without anyone typing it in, that's a FHIR-based API in operation. No manual re-entry, no phone calls — just data moving where it needs to go.
What are the four types of API?
The four types are: Open/Public APIs (accessible to any developer), Partner APIs (shared between specific organizations), Internal/Private APIs (used within a single organization to connect internal systems), and Composite APIs (bundling multiple data requests into one call). The CMS-mandated APIs — Patient Access, Provider Access, Payer-to-Payer, and Prior Authorization — are examples of standardized partner and public APIs.
What is FHIR and why does it matter for healthcare APIs?
FHIR (Fast Healthcare Interoperability Resources) is the data standard that defines how healthcare information is structured and exchanged via APIs. CMS and ONC have mandated its use across payers and health IT systems, reducing custom development costs and enabling any FHIR-compliant system to connect across the full ecosystem of payers and health IT vendors.
How do healthcare APIs improve patient outcomes?
APIs improve outcomes by ensuring care teams have complete, current patient information at every decision point. This reduces errors at care transitions and accelerates coordination of transport, prior authorization, and post-acute services — directly affecting length of stay and readmission risk.
Are healthcare APIs required by law?
Yes. CMS and ONC regulations require certain payers — including Medicare Advantage plans, Medicaid managed care, CHIP programs, and QHP issuers — to implement specific FHIR-based APIs. The 2024 CMS Interoperability and Prior Authorization Final Rule sets operational PA provisions for January 1, 2026, with full API compliance required by January 1, 2027.