Introduction
Most hospital discharge planners think of home care logistics as a scheduling function. Book the nurse, arrange the ride, confirm the equipment. Done.
That framing is exactly why patients end up back in the emergency room.
The decisions made at discharge directly determine whether a patient recovers safely at home or returns within 30 days — which caregiver visits first, whether the hospital bed arrives before the patient does, whether transport is arranged before the authorization lapses. According to a peer-reviewed study of over 786,000 Medicare beneficiaries, patients who started home health services on days 3–7 post-discharge had 28% higher odds of rehospitalization compared to those who started within 2 days. Those who waited 8–14 days faced odds more than four times higher.
That's an infrastructure failure, not a scheduling problem.
This guide covers what home care logistics actually encompasses, where coordination breaks down, how technology is closing the gap, and what high-performing agencies and health systems do differently.
Key Takeaways
- Home care logistics spans caregivers, transport, DME, and post-discharge services across multiple organizations — not just one agency's schedule
- Delayed first home visits measurably increase readmission risk and expose hospitals to value-based purchasing penalties
- AI-driven routing optimization has demonstrated cost reductions of up to 57% in peer-reviewed logistics studies
- Unifying caregivers, transport providers, DME suppliers, and payers within a single workflow eliminates the handoff gaps that drive delays
- Agencies that treat logistics as infrastructure rather than administration consistently outperform peers on clinical and financial metrics
What Is Home Care Logistics? (And Why It's More Than Scheduling)
Home care logistics is the end-to-end coordination of caregivers, transport services, durable medical equipment, and post-discharge resources needed to deliver clinical care at a patient's home.
The distinction from basic scheduling matters. Scheduling manages appointments within a single organization. Home care logistics spans multiple organizations, provider types, and data systems simultaneously.
The Infrastructure vs. Scheduling Gap
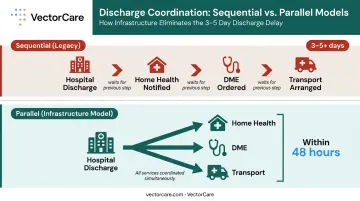
Treating logistics as a scheduling problem means every handoff becomes a separate manual process. Hospital to home health agency, agency to DME supplier, supplier to transport provider: each transition is prone to delays, miscommunications, and dropped information.
Treating it as infrastructure connects those handoffs systematically. A discharge event triggers transport coordination, DME ordering, and home health agency notification in parallel rather than sequentially.
The stakeholders involved include:
- Hospitals and discharge planners
- Home health agencies
- Non-emergency medical transport (NEMT) providers
- DME suppliers
- Medicare Advantage plans and payers
- Skilled nursing facilities (SNFs) and PACE organizations
Siloed operations across these groups create the fragmentation that drives delays. The real operational challenge isn't scheduling within a single agency: it's the broader coordination ecosystem connecting all of them. That's what scales — and what breaks — as home-based care volume grows.
Scale Makes This Urgent
According to MedPAC's 2026 Report to Congress, approximately 2.7 million fee-for-service Medicare beneficiaries received home health services in 2024, with Medicare spending $16.0 billion on those services across 12,234 certified agencies. Home-based care continues expanding, driven by aging demographics, payer preference, and patient demand. The logistics complexity grows with it.
Core Components of Home Care Logistics
Caregiver Scheduling and Matching
Caregiver scheduling goes well beyond filling time slots. Effective matching requires:
- Aligning staff certifications to patient clinical requirements
- Matching caregiver competencies to patient acuity levels
- Maintaining continuity across visits for the same patient
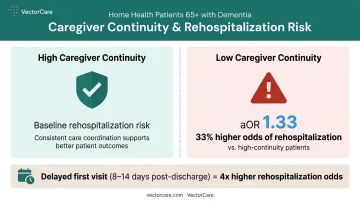
That last point carries real clinical weight. A 2021 peer-reviewed study of 23,886 adults aged 65+ with dementia receiving home health after hospitalization found that low nursing continuity was associated with 33% higher odds of rehospitalization (aOR 1.33; 95% CI 1.25–1.46) compared to high continuity. Consistent caregiver-patient pairings aren't just a patient preference — they're a readmission prevention strategy.
Route Optimization and Transport Coordination
Whether the first visit happens on time depends on two logistics decisions made before the caregiver ever leaves the building.
Route optimization determines how efficiently caregivers move between distributed patient locations. Agencies relying on manual routing or basic map tools leave significant capacity on the table — purpose-built optimization tools reduce travel time, increase daily visit capacity, and lower per-visit costs.
Post-discharge transport is one of the most commonly delayed steps in the transition. Arranging the actual move from hospital or SNF to home requires matching the transport mode (ambulance, NEMT, or ride-share) to patient acuity, under time pressure. Delays here cascade directly into delays for the first home visit.
DME Delivery and Payer Authorization
Equipment availability and payer approvals are two components that rarely make it into logistics planning — until they cause a crisis.
Patients discharged for home oxygen therapy, wound care, or mobility support cannot receive care safely without DME in place. Delays don't just inconvenience patients; they can force caregivers to abort visits or trigger emergency returns to the hospital.
Authorization timelines compound the problem. A 2025 peer-reviewed study found that 90% of Medicare Advantage enrollees were in plans requiring prior authorization for home health services, with review timelines ranging from 1–3 days to as long as a week. When authorization isn't confirmed before discharge, visit cancellations and delayed care initiation follow.
Key Challenges in Home Care Logistics
Fragmentation Across Providers
The core operational problem is structural: hospitals, home health agencies, transport providers, and DME suppliers typically operate on separate platforms with no shared data layer. The result is coordinators working through phone calls and faxes, manually following up with each vendor in sequence.
A 2025 prior authorization study put hard numbers to that friction — documenting cases where administrators spent up to 2 hours on the phone to obtain a single authorization. Multiply that across every discharge, and the cumulative administrative burden becomes staggering.
Time Pressure at Discharge
CMS defines timely initiation of care as beginning on the physician-ordered date or within 2 days of referral or inpatient discharge. Medicare Conditions of Participation require the initial assessment visit within 48 hours of referral or the patient's return home.
Meeting that window requires transport, DME delivery, and caregiver assignment to be completed nearly simultaneously. Legacy coordination processes (where each handoff is triggered only after the previous one completes) consistently miss this timeline.
Workforce Variability and Shortages
Home care agencies typically manage a mix of full-time, part-time, and contract caregivers with varying credentials. Schedulers are constantly filling around availability gaps in markets where supply is tight.
According to PHI, researchers project a shortage of 151,000 direct care workers by 2030 and 355,000 by 2040, alongside 9.7 million total direct care jobs needing to be filled over the next decade. These projections signal a permanent structural condition — not a temporary gap — and logistics systems that don't account for it will keep breaking down at the staffing layer.
Key implications for logistics coordinators:
- Credential verification must happen in real time, not at the point of scheduling
- Contingency coverage needs to be built into workflow design, not bolted on after a no-show
- Vendor networks require enough depth to absorb routine availability gaps without manual escalation
How Technology Is Transforming Home Care Logistics
From Manual Coordination to Dynamic Optimization
The performance gap between manual and technology-driven scheduling is measurable. A 2025 peer-reviewed review of home health routing and scheduling studies found simulation-based cost reductions of 45–57% across multiple tested algorithms. These are modeling results, not deployed benchmarks. Still, the conclusion holds: optimization built specifically for home health routing substantially outperforms manual methods.
AI-driven scheduling platforms move coordination from static assignment (match available caregiver to open slot) to dynamic multi-constraint optimization, accounting for geography, credentials, continuity preferences, payer requirements, and real-time availability simultaneously.

Real-Time Visibility Changes the Coordination Model
The operational difference between reactive and proactive coordination comes down to visibility. When coordinators can see caregiver locations, transport ETAs, and service status across all active patients in one view, they can intervene before a delay reaches the patient.
Most agencies still operate reactively : they learn about a problem when a patient or caregiver calls to report it. By then, the first visit may already be missed and the readmission clock is running.
VectorCare's Unified Patient Logistics Infrastructure
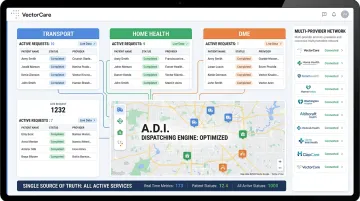
That reactive gap is exactly what infrastructure-level platforms are designed to close. VectorCare illustrates what this looks like in practice: a single ecosystem connecting transport, home health, and DME coordination rather than patching individual handoffs.
Key capabilities include:
- A.D.I. (Automated Dispatching Intelligence) automates dispatching tasks across transport, home health, and DME within one platform
- SMART on FHIR integration with Epic reduces per-discharge transport coordination from 31 minutes to under a minute
- FHIR-native architecture connects referrals across transport, DME, and home health for PACE organizations and health systems
- 100,000+ coordination hours saved for customers in 2025, across 2,500+ healthcare facilities
Performance Benchmarks: What Good Home Care Logistics Looks Like
The Metrics That Matter
Every agency and health system should track these indicators:
| Metric | What It Signals |
|---|---|
| Discharge-to-first-visit time | Readmission risk and compliance with CMS timeliness standards |
| Visit completion rate within time windows | Operational reliability and caregiver utilization |
| Average caregiver travel time per day | Route optimization effectiveness |
| 30-day readmission rate for home health patients | Aggregate logistics and clinical care quality |
The national benchmark for care initiation is within 2 days of discharge or referral, per CMS Home Health Quality Reporting Program standards. Missing this window consistently exposes agencies to HHVBP performance penalties ranging from -5% to +5% of Medicare FFS payments — which took effect in 2025.
The Financial Case for Getting This Right
Those penalty windows connect directly to the cost side of the equation. According to AHRQ's HCUP Statistical Brief #304, the average hospital readmission in 2020 cost $16,300 — exceeding the average $14,500 index admission. Medicare stays carried the highest readmission rate at 17.0 per 100 index admissions.
For hospitals under the Hospital Readmissions Reduction Program, those readmissions carry penalty exposure on top of direct costs. For home health agencies under expanded HHVBP, readmission performance now determines payment adjustments. Logistics investment, in other words, maps directly to reimbursement outcomes.
Best Practices for Optimizing Home Care Logistics
Standardize and Simultaneously Trigger the Discharge Handoff
Sequential handoffs — hospital notifies home health agency, then agency orders DME, then someone arranges transport — add days to care initiation without adding clinical value.
The better model triggers DME orders, transport coordination, and home health agency notification simultaneously at the point of discharge. This requires a defined discharge logistics protocol, not ad hoc coordination.
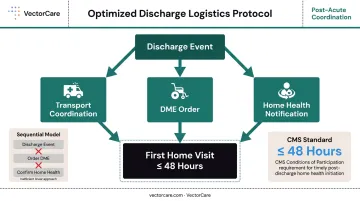
Hospitals that build this protocol into their discharge workflow rather than treating it as a post-discharge task meet the 48-hour initiation standard more reliably.
Build Feedback Loops Between Clinical and Logistics Teams
Effective logistics operations don't treat scheduling as a back-office function separate from clinical quality. They build structured connections between the two:
- Weekly logistics review meetings that surface recurring delay patterns
- Real-time exception flagging when a visit is at risk of missing its window
- Caregiver input on route feasibility and patient acuity changes
- Patient satisfaction data reviewed alongside visit completion rates
When schedulers have visibility into clinical outcomes and clinicians have visibility into logistics performance, the feedback loops that prevent avoidable failures exist. That visibility is what separates teams that catch problems early from those that keep solving the same ones.
Consolidate on Platforms That Bridge Silos
A frequent technology mistake in home care logistics is accumulating point solutions — one tool for caregiver scheduling, another for transport, a third for DME tracking — each solving one piece of the problem in isolation.
When evaluating logistics technology, prioritize platforms that offer:
- EHR integration via FHIR standards (not manual data exports)
- Multi-provider network connectivity across transport, DME, and home health
- Automated dispatching that removes manual assignment steps
- Real-time visibility across all active service types
VectorCare's platform connects these coordination layers within a single HIPAA-secure environment — with FHIR-based EHR integration, automated dispatching through its A.D.I. engine, and a multi-provider network spanning transport, home health, and DME. For health systems managing high discharge volumes, that means fewer manual handoffs and a single source of truth across every active service type.
Frequently Asked Questions
What does home care logistics do?
Home care logistics coordinates caregivers, transport, DME, and post-discharge services to ensure patients receive timely, appropriate care at home. When done well, it reduces hospital readmissions and improves recovery outcomes by closing the coordination gaps that develop between discharge and the first home visit.
How does home care logistics differ from standard patient scheduling?
Standard scheduling manages appointments within a single care setting. Home care logistics coordinates multiple providers — transport companies, DME suppliers, home health agencies, and payers — across a distributed, multi-organization network where no single entity controls all the moving parts.
What role does technology play in improving home care logistics?
AI-driven platforms automate multi-constraint scheduling, optimize caregiver routes, and provide real-time visibility across providers. EHR integration eliminates manual data re-entry — cutting communication-related delays by 45% and improving on-time visit performance.
How does poor home care logistics affect patient outcomes?
Delays in post-discharge visits, equipment delivery, or caregiver assignment increase readmission risk and can trigger safety incidents. A missed 48-hour initiation window more than quadruples rehospitalization odds when the delay extends to 8–14 days.
What should hospitals look for in a home care logistics platform?
Look for multi-provider network connectivity, FHIR-based EHR integration, automated dispatching, and real-time tracking across transport, DME, and home health. Point solutions that cover only one coordination layer tend to create new silos rather than solve existing ones.
How does home care logistics help reduce hospital readmissions?
Timely first home visits, coordinated DME delivery, and consistent caregiver follow-up are among the most evidence-supported interventions for preventing 30-day readmissions. Each of these outcomes depends on logistics execution — not just clinical quality — making logistics infrastructure a direct lever on readmission rates.