This guide is written for home health agencies, hospital discharge planners, and care coordinators — the people responsible for one of healthcare's most consequential handoff points. We cover what discharge instructions must include, how the end-to-end process works, where agencies consistently fall short, and what it takes to close the gaps before the final visit.
Key Takeaways
- Discharge instructions are a CMS compliance requirement under 42 CFR Part 484— agencies that skip or rush them face both regulatory exposure and measurable outcome penalties.
- Effective instructions cover medications, warning signs, care routines, confirmed follow-up appointments, and DME already in place.
- CMS national data puts the potentially preventable 30-day post-discharge readmission rate at 4.12% — a direct measure of discharge process failure.
- Agencies that treat discharge as a last-visit task — rather than starting at admission — consistently report worse outcomes and lower CAHPS scores.
- Logistics gaps — missing transportation, delayed DME, unscheduled follow-ups — are where most discharge plans actually break down.
What Are Home Health Discharge Instructions?
Home health discharge instructions are the formal directions issued when a patient completes their certified home health episode and transitions to self-managed care, community support, or a lower-intensity service level. This is not the same paperwork a patient receives when leaving a hospital.
A hospital discharge sends a patient to home health. A home health discharge sends a patient away from skilled professional care — or into a setting where visits are less frequent and clinical oversight is minimal. That's a meaningful difference in what the documentation needs to accomplish.
The process is governed by CMS Conditions of Participation under 42 CFR Part 484, specifically:
- 484.50 — Patient rights, including written notice requirements
- 484.55 — Comprehensive assessment, including medication review
- 484.58 — Discharge planning
- 484.60 — Care planning, coordination, and patient/caregiver education
- 484.110 — Clinical records, including the discharge summary
Home health discharge instructions serve two purposes at once: they prepare patients for independent recovery and satisfy a compliance requirement with firm documentation deadlines. The discharge summary must reach the primary care practitioner within 5 business days of discharge — a clock that starts the moment the episode closes.
Why Discharge Instructions Are Critical in Home Health
The stakes are measurable. CMS national home health data shows that while 77.71% of home health patients are successfully discharged to the community, 10.83% experience a potentially preventable hospitalization during their home health stay — meaning the discharge problem begins well before the final visit.
Discharge planning cannot wait until the episode is nearly over. Patients hospitalized mid-episode were typically showing warning signs earlier — signs that weren't caught or acted on in time.
The HHVBP Connection
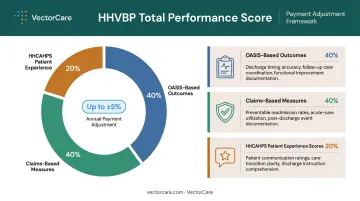
Weak discharge instruction processes don't just harm patients. They affect agency finances directly. Under the expanded Home Health Value-Based Purchasing model, CMS applies up to a 5% upward or downward payment adjustment based on a Total Performance Score weighted:
- 40% OASIS-based outcomes
- 40% claims-based measures (including preventable readmissions and hospitalizations)
- 20% HHCAHPS patient experience scores
All three categories trace back to discharge execution: poor medication reconciliation hits OASIS outcomes, preventable readmissions surface in claims data, and patients who couldn't follow their instructions drag down HHCAHPS scores.
What Goes Wrong Without Adequate Instructions
The same failures repeat across agencies:
- Patients mismanage medications because no one reconciled the changes made during the episode
- Caregivers don't recognize warning signs because instructions were written in clinical jargon
- Follow-up appointments are missed because they were "recommended" rather than scheduled
- Equipment isn't in place because delivery wasn't confirmed before the final visit
- Patients call 911 because they have no escalation pathway and don't know who else to call
What Should Be Included in Home Health Discharge Instructions
CMS does not publish a single universal template, but the required elements are distributed across the Conditions of Participation. Every discharge instruction set should cover five domains.
Medications and Reconciliation
Medication reconciliation is the highest-risk component of any discharge. Patients transitioning off skilled care must understand every medication: name, dose, timing, route, purpose, and any changes made during the home health episode.
The discharge document must reconcile the current medication list against what the patient was taking before the episode began. Per the Joint Commission's 2025 home care National Patient Safety Goal NPSG.03.06.01, this means identifying and resolving discrepancies such as omissions or duplications, and providing written medication information to the patient or caregiver.
Key elements to document:
- Full medication list with dose, frequency, and route
- Any medications added, changed, or discontinued during the episode
- Side effects to watch for
- Who to contact if there's a question or discrepancy
Warning Signs and When to Call
Warning signs must be condition-specific and written in plain language — no clinical abbreviations, no generic checklists. A cardiac patient needs different red flags than a wound care patient.
A complete warning signs section identifies:
- Specific symptoms requiring a provider call (fever above a threshold, wound drainage changes, swelling)
- Symptoms requiring immediate emergency care (chest pain, sudden confusion, difficulty breathing)
- The exact phone number to call, not just "contact your doctor"
Care Routines and Activity Guidelines
Discharge instructions must clearly state what the patient can and cannot do independently. This includes activity restrictions, weight-bearing limits, wound care protocols, dietary requirements, and any equipment-dependent self-care routines.
For patients with active caregiver support, instructions should address the caregiver directly. That means specifying:
- What tasks the caregiver is expected to manage day-to-day
- How to perform any hands-on care procedures
- What the escalation path looks like if something changes
Follow-Up Appointments and Referrals
Appointments should be confirmed, not recommended. There is a meaningful difference between writing "schedule follow-up with PCP within 7 days" and listing the actual appointment date, time, location, and provider name.
Discharge instructions should also confirm:
- Transportation is arranged for each appointment
- Specialist and outpatient therapy referrals are active, not pending
- The patient knows what to do if they need to reschedule
Skipped follow-up appointments are directly linked to preventable readmissions. Transportation is the leading non-clinical barrier — particularly for Medicaid beneficiaries and elderly patients who lack reliable access to a vehicle or driver.
DME, Supplies, and Community Resources
Equipment must be in place before the final skilled visit. Confirming that a hospital bed, walker, or oxygen concentrator has been ordered is not the same as confirming it has been delivered, is functioning, and the patient knows how to use it.
Discharge instructions should also document:
- Any ongoing non-skilled home care services confirmed and scheduled
- Referrals to community resources, meal programs, or caregiver support organizations
- Who is responsible for managing supply reorders
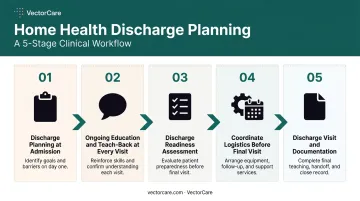
How the Home Health Discharge Process Works
The discharge process is not a single event. It is an ongoing process that begins at the start of care and concludes with a formal discharge visit.
Step 1: Discharge Planning Begins at Admission
Best practice — including the IDEAL framework developed by AHRQ — requires discharge goals to be set at intake. From day one, clinicians should document:
- Expected discharge outcomes
- Patient and caregiver education milestones
- Potential barriers to independent self-management (cognitive limitations, caregiver availability, housing issues, transportation access)
Agencies that start discharge planning at admission have a roadmap. Agencies that skip this step arrive at discharge without a plan — and patients feel the difference.
Step 2: Ongoing Education and Teach-Back at Every Visit
At each skilled visit, clinicians reinforce patient education on medications, condition management, and warning signs. The standard for confirming understanding is teach-back methodology — asking patients and caregivers to explain or demonstrate what they learned in their own words.
Used correctly, teach-back surfaces misunderstandings before they become medical events. Every session should be documented in the clinical record — it supports HHCAHPS scores and satisfies the ongoing education requirements under 42 CFR 484.60.
Step 3: Discharge Readiness Assessment
The clinical and interdisciplinary team evaluates each of the following before a discharge date is confirmed:
- Patient functional status and stability
- OASIS discharge items (using M0100 Reason for Assessment 09 under OASIS-E1, effective January 1, 2025)
- Caregiver capability and confidence
- Outstanding barriers — unresolved wound care, equipment gaps, training deficits
Don't set a discharge date until each item is resolved or has a documented plan.
Step 4: Coordinating the Logistics Before the Final Visit
Instructions only work if the logistics behind them are operational. That means completing each of the following before the final visit:
- Follow-up appointments must be scheduled, not recommended
- DME must be delivered and confirmed functional
- Transportation for appointments must be arranged
- Community referrals must be active
This coordination layer is where most discharge failures actually happen. Fragmented communication between the home health agency, referring physician, DME supplier, and transportation provider creates gaps that no instruction document can close on its own.

Platforms like VectorCare help home health agencies and hospitals close this gap by coordinating transportation, DME dispatch, and provider communication within a single system — including pre-discharge scheduling of follow-up appointment rides so transportation is confirmed before the patient is formally discharged.
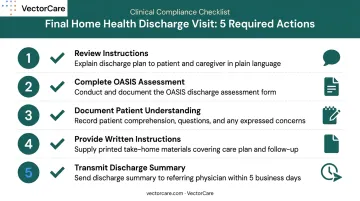
Step 5: The Discharge Visit and Documentation
At the final visit, the clinician:
- Reviews all discharge instructions with the patient and caregiver in plain language
- Completes the OASIS discharge assessment
- Documents the patient's understanding and any outstanding concerns
- Provides written instructions the patient can reference at home
- Ensures the referring physician receives a discharge summary within 5 business days
The written instructions and the clinician-facing discharge summary should be aligned — patients should not receive information that conflicts with what the provider receives.
Common Gaps and Misconceptions in Discharge Instruction Delivery
The Last-Visit Trap
The most common incorrect assumption in home health is that discharge planning is a task for the final visit. Agencies that treat discharge instructions as end-of-episode paperwork consistently see higher readmission rates and lower CAHPS scores than those that integrate discharge education across every clinical encounter.
Compressing all discharge education into one visit creates two problems: there is not enough time to cover everything adequately, and there is no opportunity to catch and correct misunderstanding before the patient is on their own.
Generic Forms Are Not Discharge Instructions
CMS requires individualized plan-of-care content. A pre-printed discharge form that lists generic warning signs or a standard medication schedule does not meet that standard — and it does not serve the patient.
A generic handout may look complete. It rarely prepares a patient for independent recovery. Three critical elements cannot be pre-printed — they have to be built for each patient:
- Condition-specific warning signs
- Reconciled medication lists
- Confirmed follow-up appointments
Delivery Is Not the Same as Understanding
Handing a patient a discharge packet at the final visit is not effective discharge instruction. It is paperwork delivery.
Effective discharge instruction requires:
- Documented teach-back confirming the patient can explain their instructions
- Confirmed caregiver readiness and capability
- Verified logistics — appointments scheduled, equipment in place, transportation arranged
Misinterpreting instruction delivery as instruction comprehension is a systemic gap across home health agencies, and it shows up directly in HHCAHPS patient experience scores.
Conclusion
Home health discharge instructions are the formal mechanism that closes a skilled care episode safely. They prepare patients and caregivers to maintain recovery independently, and they ensure the clinical and logistical continuity needed to prevent avoidable readmissions.
Discharge planning only works when it runs as a continuous care function, not a final-visit formality. That means:
- Starting the discharge plan at admission, not at the end of the episode
- Reinforcing patient education through every visit using teach-back
- Confirming follow-up appointments and DME delivery before the last visit closes
- Verifying caregiver competency in writing before the agency exits the case
When agencies treat discharge as a back-office checklist, the resulting care gaps are neither inevitable nor acceptable. The clinical and logistical groundwork described in this guide exists precisely to close those gaps before they become readmissions.
Frequently Asked Questions
How do you discharge a patient from home health?
A clinician assesses discharge readiness, completes the OASIS discharge assessment using M0100 Reason for Assessment 09, reviews all instructions with the patient and caregiver using plain language, and formally closes the episode. The discharge summary must reach the primary care practitioner within 5 business days.
What should be included in home health discharge instructions?
The five core components are: medication reconciliation, condition-specific warning signs in plain language, care routines and activity guidelines, confirmed follow-up appointments with transportation arranged, and DME and community resources already in place before the final visit.
What is the IDEAL discharge planning framework?
IDEAL is an AHRQ framework for hospital-to-home transitions. The acronym covers including patients and families as partners, discussing medications and warning signs, educating in plain language, assessing understanding through teach-back, and listening to patient goals. Home health clinicians use it to guide discharge teaching conversations.
Who is responsible for creating home health discharge instructions?
The primary clinician — typically a registered nurse or therapist — is responsible for completing and documenting discharge instructions, with input from the interdisciplinary team. The referring physician receives a copy of the discharge summary to maintain care continuity after the episode closes.
What are the most common reasons patients are readmitted after home health discharge?
The primary drivers are medication mismanagement, failure to recognize warning signs, missed follow-up appointments, inadequate caregiver training, and absent or delayed DME and community support at the time of discharge.
How long does the home health discharge process take?
The process should span the entire episode, not just the final visit. Visit length varies based on patient complexity, medication burden, and caregiver readiness. The OASIS discharge assessment and summary must be transmitted within 5 business days of discharge.