Introduction
Healthcare organizations in 2026 are managing a growing set of operational pressures: rising patient volumes, persistent staffing shortages, and an administrative burden that pulls clinicians away from the work they trained to do. The systems meant to support care delivery — scheduling, documentation, billing, transport coordination — are often fragmented, manual, and slow.
The numbers make the stakes clear. Administrative expenses across 5,639 U.S. hospitals totaled $166.1 billion, representing 17% of total hospital spending. Meanwhile, physician burnout remains at 45% and hospital staff turnover sits at 18.3% — making it clear that adding headcount alone won't fix the underlying infrastructure problems.
This guide covers the major categories of healthcare workflow software in 2026. It makes the case for why patient logistics is the most underinvested layer in that stack — and outlines what to look for when selecting solutions that deliver measurable results.
Key Takeaways
- Administrative expenses consume 17% of total U.S. hospital spending — workflow automation is a financial necessity
- Effective healthcare software covers clinical documentation, revenue cycle, scheduling, decision support, and patient logistics
- Patient logistics — transport, NEMT, discharge coordination — is the most overlooked high-impact workflow domain
- FHIR-based EHR integration and AI-driven automation separate high-performing platforms from the rest in 2026
- Workflow analysis — not software selection — is the right starting point for successful implementation
Why Healthcare Workflows Need an Upgrade in 2026
The core problem isn't a shortage of technology — it's a surplus of disconnected systems.
Most hospitals still operate across incompatible tools: phone calls to arrange transport, faxes for DME orders, siloed EHRs that don't communicate with scheduling or billing platforms. Every manual handoff between systems is a potential delay, error, or staff hour burned on coordination instead of care.
The Workforce Can't Absorb More Manual Work
With hospital RN vacancy rates at 9.9% and overall staff turnover at 18.3%, the margin for inefficiency has disappeared. When transport coordinators spend 31 minutes arranging a single patient transfer by phone, or billing staff manually review claims that automation could handle in seconds, the system fails — not because of effort, but because of infrastructure.
The clinical workflow solutions market reflects this urgency: valued at $13.36 billion in 2025 and projected to reach $26.25 billion by 2031 at an 11.92% CAGR. That growth signals an industry finally treating workflow software as infrastructure — not overhead. The real question is which solutions address root causes rather than symptoms.
Infrastructure Problems Require Infrastructure Solutions
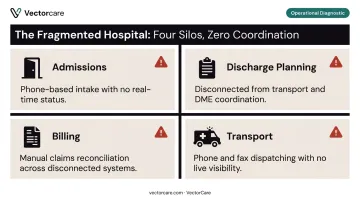
Staffing additions and process tweaks don't fix broken infrastructure. When the core systems across a care continuum operate in silos, no amount of headcount fully compensates. Fragmentation shows up everywhere:
- Admissions relying on phone-based intake with no real-time status
- Discharge planning disconnected from transport coordination and DME orders
- Billing manually reconciling claims that integrated platforms could auto-process
- Transport dispatched through calls and faxes instead of automated workflows
The organizations making the most progress in 2026 are treating their workflow software stack as core operational infrastructure — not a collection of departmental tools.
Key Categories of Healthcare Workflow Software in 2026
Clinical Documentation and EHR Automation
Documentation burden is one of the primary drivers of clinician burnout. Ambient AI scribes — which listen during patient encounters and automatically generate clinical notes — are changing that equation fast.
The evidence is concrete: The Permanente Medical Group deployed ambient AI scribes that were used 2.5 million times and saved 15,791 documentation hours over 63 weeks. A peer-reviewed JAMA Network Open study of 263 clinicians found burnout dropped from 51.9% to 38.8% after just 30 days of use, with after-hours documentation time falling by nearly an hour per day.
Key capabilities in this category:
- Ambient AI scribes that generate structured notes from natural conversation
- Smart templates that auto-populate based on diagnosis codes or visit type
- Automated EHR data entry that pulls from previous encounters and labs
Revenue Cycle and Billing Automation
According to HFMA-FinThrive research, 63% of healthcare organizations now use AI and automation in revenue cycle functions. This includes claim scrubbing, AI-assisted coding, denial management, and prior authorization processing.
Prior authorization deserves specific attention: the AMA's 2024 survey found 93% of physicians say prior authorization delays access to necessary care. That's not just a billing inefficiency. It's a patient outcome risk. Platforms that automate prior auth workflows reduce both administrative friction and clinical harm.
Patient Scheduling, Intake, and Communication
92% of consumers want to schedule appointments online, yet actual online booking shares in clinical settings run as low as 7-22% depending on the practice type. That gap represents significant untapped efficiency.
Automated scheduling platforms close it by offering:
- Digital intake forms that sync directly to the EHR
- Appointment reminders via SMS and email
- Self-scheduling portals that reduce front-desk call volume
- Risk-stratified outreach for high no-show patients
The data on no-show reduction is nuanced: online scheduling reduces no-shows in some settings but not all. The strongest results come from combining automated reminders with targeted outreach for high-risk appointments.
Clinical Decision Support
71% of U.S. acute care hospitals now use predictive AI integrated with their EHRs — up from 66% in 2023. These tools surface real-time alerts for sepsis risk, readmission probability, and patient deterioration directly within clinical workflows.
The evaluation challenge cuts deeper than adoption rates. 90% of hospitals using the leading EHR vendor have adopted this capability, compared to 50% using others — and that vendor concentration creates real governance risk. When selecting CDS tools, require transparency into:
- How models are trained and validated
- How they are monitored after deployment
- What populations the training data represents
Patient Logistics and Transport Coordination
This is the category most often misclassified as a scheduling function. It isn't. Inter-facility transfers, NEMT coordination, home health referrals, and discharge planning involve multi-party orchestration across dozens of providers. Failures in this coordination layer drive bed blockage, extended length of stay, and direct clinical complications — costs that don't show up on a scheduling report but do show up in outcomes data.
Patient Logistics: The Overlooked Workflow That Impacts Everything
When a patient is medically ready for discharge but can't leave because transport hasn't been arranged, DME hasn't been delivered, or a home health agency hasn't confirmed intake — that's not a scheduling failure. That's an infrastructure failure.
Nearly 20% of patients experience adverse events within three weeks of discharge, and three-quarters of those events are considered preventable. Delayed discharges increase complication risk and drive up costs across the entire system.
The manual burden compounds the problem. A 2025 literature review confirmed that hospital transport staff travel up to 18 miles per day managing logistics still handled, in many facilities, by phone.
What Unautomated Patient Logistics Actually Looks Like
A typical discharge coordination sequence without dedicated logistics software:
- Care coordinator identifies patient is ready for discharge
- Calls transport provider — often waiting on hold or leaving voicemail
- Manually negotiates time and price
- Calls DME supplier separately
- Faxes home health referral
- Repeats calls for status updates with no visibility into progress
- Repeats this for 25+ patients per day
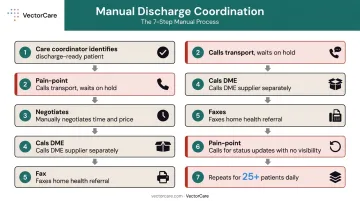
Each transport request averages 31 minutes of manual coordination time. For a 250-bed hospital managing 25 daily transports, that's over 4,700 staff hours per year — before accounting for errors, cancellations, and missed handoffs.
That's the operational cost of treating logistics as a scheduling problem. VectorCare was built to address it as the infrastructure problem it actually is.
How VectorCare Solves the Patient Logistics Infrastructure Problem
VectorCare is purpose-built for this layer of healthcare operations — a platform that connects transport coordination, NEMT, home health referrals, DME ordering, and discharge planning in one automated system.
Key capabilities:
- SMART on FHIR integration with Epic: Patient vitals, weight, and demographics auto-extract when a coordinator initiates a transfer request inside Epic — no duplicate data entry, no toggling between systems. Transfer coordination that previously took 35 minutes drops to 90-second decision cycles.
- Automated dispatch network: Fulfillment requests are broadcast to a network of credentialed transport providers, who respond in real time. No sequential phone calls, no manual negotiation.
- Real-time ETA visibility: Nursing staff and care coordinators receive automated notifications and delay alerts with no follow-up calls required.
- One platform, five workflows replaced: Ambulance transfers, wheelchair van services, NEMT, home health coordination, and DME delivery all run through a single system — eliminating parallel phone-and-fax processes.
The platform serves over 2,500 healthcare facilities nationwide. In its first six weeks of deployment across four air operators and two hospital networks, VectorCare processed 847 transfer requests. The Orange County Health Care Agency reduced mental health crisis transport coordination from 45 minutes to under 5 minutes — roughly a 10x time savings.
The Financial Case
VectorCare partner hospitals average over $500,000 in annual savings, driven primarily by two cost categories:
| Savings Driver | Mechanism |
|---|---|
| Labor (scheduling time) | 31 min/request → under 3 min/request |
| Bed utilization | Faster discharge coordination frees capacity |
| ALS/BLS optimization | Appropriate dispatch reduces high-cost transport overuse |
| Reduced readmissions | Better logistics supports timely follow-up care |
One California health system managing over 900,000 service requests annually saved $22.2 million from scheduling time reduction alone. For high-volume systems, $500,000 is a conservative floor.
What to Look for in Healthcare Workflow Software in 2026
Not every platform marketed as "healthcare workflow software" is built for the complexity of real care coordination. Three requirements separate serious contenders from the rest.
HIPAA Compliance and Security Architecture
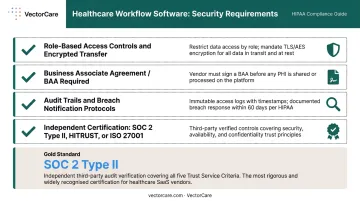
Any platform handling protected health information must provide:
- Role-based access controls and encrypted data transfer
- Formal Business Associate Agreement (BAA) — required by HHS for all PHI-handling vendors
- Audit trails and breach notification protocols
- Independent security assurance (SOC 2 Type II, HITRUST, or ISO 27001)
VectorCare, for example, holds SOC 2 Type II certification alongside HIPAA compliance — a meaningful distinction, since SOC 2 Type II requires third-party auditors to verify that controls are operating consistently over time, not just designed correctly.
EHR Integration Depth
Generic API connections aren't enough. Evaluate whether a platform uses HL7 FHIR or SMART on FHIR standards to embed natively within your existing EHR.
ONC data shows FHIR-based API adoption grew from 62% of hospitals in 2021 to 74% in 2024 — the ecosystem is ready. Deeper integration eliminates duplicate data entry, reduces transcription errors, and ensures workflow software extends the EHR rather than working around it.
Automation Intelligence and No-Code Flexibility
The distinction between rule-based routing and genuine AI-driven automation matters in practice. Look for:
- Real-time event triggers (not batch processing)
- Adaptive dispatch or scheduling logic
- No-code workflow configuration so administrators can modify workflows without IT backlogs
When care delivery models change, a six-month IT cycle to update a workflow isn't a bottleneck — it's a liability. Platforms built for no-code reconfiguration give administrators the flexibility to adapt the same afternoon a new protocol takes effect.
Best Practices for Implementing Healthcare Workflow Software
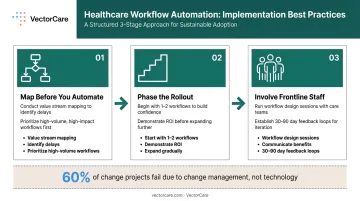
Map Before You Automate
Value stream mapping — documenting how work actually flows, where delays occur, and where manual handoffs multiply — should precede any software selection. Automating a broken process makes it faster and more expensive. Prioritize workflows with the highest volume, the most error risk, or the greatest impact on patient throughput.
Phase the Rollout
Start with one or two high-impact workflows — patient intake, discharge logistics, or transport coordination. Demonstrate ROI and build staff confidence before expanding to adjacent processes. A phased approach also gives IT and clinical teams the chance to learn what works before scaling the rollout.
Involve Frontline Staff from Day One
Healthcare IT implementation failures trace back to poor change management more often than poor software. Studies on hospital digital transformation consistently find that up to 60% of change projects fail due to change management breakdowns, not technology gaps.
Practical steps that reduce this risk:
- Engage frontline users in workflow design sessions before go-live
- Communicate concrete benefits: fewer repetitive tasks, fewer errors, more time for patients
- Create feedback loops in the first 30-90 days so staff can flag friction points before they calcify into workarounds
Frequently Asked Questions
Which software is best for a hospital management system?
Large systems typically rely on comprehensive EHR platforms like Epic or Oracle Health for clinical workflows, while operational functions — revenue cycle, patient logistics, staffing — require specialized platforms that integrate with the EHR rather than replacing it. The right fit depends on your organization's size and clinical complexity.
What is an EHR workflow?
An EHR workflow is the sequence of steps a clinical or administrative team follows within an Electronic Health Record to complete a care task — ordering labs, documenting a visit, or routing a referral. EHR workflow automation uses AI and smart templates to reduce the manual steps within those sequences.
What is healthcare workflow automation?
Healthcare workflow automation uses digital tools, AI, and system integrations to replace manual, repetitive steps in clinical and administrative processes — from appointment reminders and claims processing to patient transport coordination — reducing errors, cutting costs, and freeing staff for higher-value work.
How does patient logistics software improve hospital workflows?
Patient logistics software replaces phone and fax-based coordination for transport, NEMT, and discharge planning with real-time digital workflows. The result: reduced length of stay, faster bed turnover, and live visibility into patient movement across the care continuum — without staff fielding dozens of calls per shift.
What should healthcare organizations look for when choosing workflow software?
Prioritize these three criteria before committing to any platform:
- HIPAA compliance — formal BAA and independent security certification required
- Native EHR integration — FHIR standards, not just generic APIs
- No-code automation — so administrators can adapt workflows without waiting on IT
How does AI improve healthcare workflows in 2026?
AI improves healthcare workflows through ambient clinical documentation, predictive risk scoring, intelligent dispatch, automated coding, and real-time operational analytics — helping care teams make faster decisions and cut manual coordination without adding headcount.