Inefficient workflows delay care, exhaust staff, and drive up costs that few organizations have fully measured. When a nurse spends 30 minutes chasing down a transport confirmation instead of being at the bedside, or when a patient occupies a bed for two extra days because discharge coordination stalled, the ripple effects touch every part of hospital operations.
This article covers why hospital workflows break down, which improvement strategies produce real results, and why patient logistics — typically treated as an afterthought — is one of the highest-leverage areas to fix first.
Key Takeaways
- Delayed discharges cost hospitals an estimated $8,000–$12,000 per avoidable bed-day, with compounding effects on capacity and revenue
- Identify bottlenecks before applying fixes — generic process overhauls without diagnosis rarely produce lasting results
- Patient logistics and transport coordination are among the most underaddressed operational inefficiencies in hospital settings
- Automation reduces manual coordination only when matched to existing workflows — deploying it on broken processes compounds the problem
- Sustainable improvement requires ongoing measurement, governance, and frontline buy-in, not one-time change projects
Why Hospital Workflows Break Down (and What It Costs)
What a Hospital Workflow Actually Is
A hospital workflow is the sequence of tasks, information handoffs, and decisions that move a patient — or a clinical service — from one point to the next. That includes admissions, diagnostic orders, care transitions, discharge coordination, and everything in between. These sequences cross department boundaries, involve multiple roles, and depend on systems that often don't communicate with each other.
The problem isn't that hospitals lack processes. It's that most of those processes evolved organically — patched together over time rather than intentionally designed — and they show it.
The Root Causes
Three patterns appear consistently across healthcare systems that struggle with workflow:
- Siloed departments that hold information locally rather than sharing it in real time
- Manual communication tools — fax, pager, landline — that create delays and leave no documented trail
- Handoffs designed around convenience rather than continuity, particularly at care transitions like ED-to-inpatient or hospital-to-post-acute
Handoffs are where the most visible damage occurs. According to AHRQ PSNet, 70% of hospital-to-home transitions contain at least one safety issue, including incomplete information or medication discrepancies. A structured I-PASS handoff tool in a pediatric ED cut perceived loss of key patient information from 75% to 37.5% — a result that directly reduces downstream care gaps and bed-holding delays.
The Staff and Financial Cost
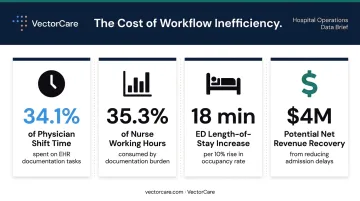
Documentation and coordination tasks pull clinical staff away from patients at a scale most administrators underestimate. A systematic review of physician EHR interaction found hospitalists averaged 34.1% of shift time on EHR tasks, with some inpatient clinicians spending 3.8 hours per day managing records.
Nurses face a parallel drain. A 36-hospital time-motion study found they spent:
- 35.3% of practice time on documentation
- 20.6% on care coordination
Neither category counts as direct patient care.
The financial consequences follow the same pattern. A 2024 analysis found that a 10% increase in hospital occupancy correlates with an 18-minute increase in ED length of stay — a clear signal of how discharge delays cascade through the whole system. Reducing admission delays to under 120 minutes could allow a hospital to accommodate 3,175 additional patient encounters annually, generating nearly $4 million in net revenue.
Proven Strategies to Improve Hospital Workflow
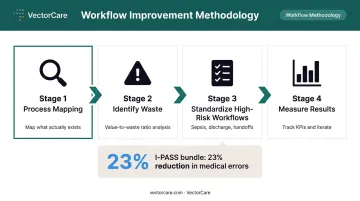
Start With Process Mapping
Before changing anything, map what actually exists. Most organizations discover their documented processes and their real workflows don't match.
Value stream mapping is the tool most supported by evidence. A 2017 systematic review found it reduced non-value-added time in 7 of 8 studies and reduced length of stay in 7 of 9 studies. In one four-hospital UK study of emergency medical care, patient journeys had an average value-to-waste ratio of 45.5%, with waits for diagnostic results accounting for 30–39% of waste time.
The critical rule: include frontline staff in the mapping process. They see the workarounds and informal processes that don't appear in any policy document. Without their input, the map you create will be as incomplete as the workflow you're trying to fix.
Standardize High-Risk, High-Volume Workflows First
Once you know where the gaps are, prioritization matters. Start with workflows that are both high-volume and high-consequence: sepsis protocols, discharge checklists, lab result communication, ED-to-inpatient handoffs.
The evidence for structured handoffs is strong. A NEJM multicenter study across nine pediatric residency programs and 10,740 admissions found the I-PASS handoff bundle reduced medical errors by 23% and preventable adverse events by 30%.
Standardization doesn't eliminate clinical judgment. It protects against critical steps being skipped when a different nurse is on duty, a shift change happens mid-transfer, or a unit is operating at full capacity.
Redesign Communication Systems
Outdated communication tools are often the easiest early win. Replacing pagers and fax-based communication with secure messaging creates a documented, traceable record and ends the phone tag that slows clinical teams down.
In a large urban academic safety-net hospital, adding secure messaging to a unidirectional paging system cut the median daily potential communication failure rate from 5.5% to 2.2% (a 59% decrease). Monthly message volume grew from roughly 9,000 in 2018 to nearly 379,000 by early 2022, reflecting genuine adoption rather than compliance-only usage.
Closed-loop communication takes this further: an alert isn't considered complete until the receiving clinician confirms receipt. A four-year study of an automated critical imaging alert system found adherence improved from 91.3% to 95.0%, with system-routed alerts reaching 97.9% adherence.
Worth noting: 41% of total alerts used asynchronous notification for less urgent results, reducing unnecessary interruptions without sacrificing accountability.
Involve All Stakeholders in Redesign
Workflow changes fail when one department designs them in isolation. The most durable improvements involve cross-functional teams (clinicians, nurses, case managers, IT, and administration) who understand how their workflows create downstream effects for each other.
When frontline staff are involved in the design process, adoption follows more naturally. In one nursing quality improvement collaborative, 90% of unit-based teams successfully conducted tests of change, and 46% of innovations were sustained long term — a significantly higher sustainability rate than top-down implementation typically achieves.
Patient Logistics: The Workflow Bottleneck Hospitals Overlook
Why Logistics Gets Treated as a Scheduling Task
Patient logistics — the coordination of transport, interfacility transfers, home health setup, DME delivery, and post-acute placement — is one of the most workflow-intensive parts of hospital operations. Most hospitals still manage it through phone calls, manual dispatching, and spreadsheets.
This is a structural mismatch. Logistics isn't a scheduling task. It's the connective infrastructure that links the hospital to post-acute facilities, home health agencies, and transport providers. When it breaks, the backlog affects bed availability, care capacity, and the ability to accept new patients.
The Specific Workflow Costs of Manual Logistics
Three operational costs stand out:
- Traditional manual transport dispatch had an overtime delay rate of 41.0% in one 2024 hospital transport study — an IoT-based dispatch system reduced that to 26.5%
- Transport coordination using legacy phone-and-fax workflows averages approximately 31 minutes per ride request — time spent by care coordinators, discharge planners, or case managers who could be doing other work
- Delayed discharges driven by unconfirmed or uncoordinated transport keep beds occupied longer than clinically necessary, compressing capacity throughout the facility
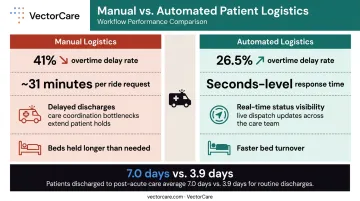
Patients discharged to post-acute care settings already have average lengths of stay nearly twice those of routine discharges (7.0 days vs. 3.9 days, per AHRQ HCUP data). Every hour of unresolved logistics adds to that gap.
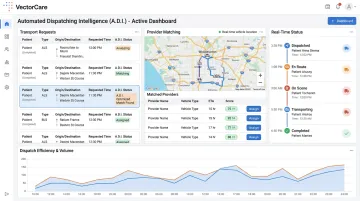
Real-Time Visibility Changes the Equation
When a care team can see exactly where a transport request stands — whether a provider has accepted, when a patient will arrive, when discharge has been completed — redundant follow-up calls stop. Care teams can plan transitions instead of reacting to them.
Platforms like VectorCare address this directly. Through SMART on FHIR integration with Epic and other major EHR systems, transport requests are initiated from within the patient chart, with patient demographics and clinical details auto-populated, eliminating manual data entry. Requests broadcast simultaneously to available providers, with response times documented in seconds rather than minutes.
VectorCare's Automated Dispatching Intelligence (A.D.I.) handles routine triggers automatically — dispatching, provider matching, and status tracking — without coordinator intervention. In 2024 alone, A.D.I. saved customers over 10,000 hours across those tasks.
For hospitals managing dozens or hundreds of discharges daily, that adds up to a meaningful reduction in coordinator time per discharge — time that can be redirected to patients rather than phone queues.
How Technology and Automation Drive Workflow Improvement
Match Technology to Workflow, Not the Reverse
The most consistent cause of failed health IT implementation is deploying technology before analyzing the workflows it will touch. AHRQ's guidance on EHR unintended consequences explicitly identifies "more or new work," workflow disruption, and altered communication patterns as predictable outcomes when technology is layered onto unmapped processes.
The principle is straightforward: a tool that doesn't fit how people actually work creates workarounds, not improvements. Process mapping should precede any technology selection.
What Automation Actually Handles Well
Rules-based automation performs well on routine, high-volume triggers:
- Sending a transport request when a discharge order is entered
- Alerting a care team when patient status changes
- Documenting coordination steps without manual entry
- Flagging billing discrepancies against completed trip records
AI-assisted tools extend this to more complex coordination — scheduling, provider matching, negotiating times across a vendor network. In 2025, VectorCare's A.D.I. saved healthcare systems and suppliers more than 100,000 hours of administrative work by automating these dispatching and scheduling decisions at scale.
Interoperability Is Non-Negotiable
Workflow improvement tools that don't integrate with existing EHR systems create new silos. FHIR-based integration — which VectorCare supports through its SMART on FHIR certification — allows patient data to flow between systems without manual reconciliation.
When a coordinator submits a transport request from within Epic, patient vitals, demographics, and encounter details are already populated. The coordination completes, the record updates, and the care team sees status in real time — no phone calls, no parallel spreadsheets. For hospitals managing dozens of transports daily, that reduction in reconciliation time adds up fast.
Building a Culture of Continuous Workflow Improvement
Define Your KPIs Before You Change Anything
Establish baseline metrics before implementing changes. Without them, you can't distinguish actual improvement from perceived improvement — and you'll have no way to defend the next round of changes.
Key workflow KPIs to track:
- Average patient length of stay
- Discharge delays (IHI defines a delay as more than 2 hours post-order)
- Door-to-physician time in the ED
- Transport wait times and overtime delay rates
- Staff time spent on manual coordination tasks
- 30-day readmission rates
Governance matters too. A standing workflow committee — including clinical, operational, and IT representation — that reviews performance data on a regular cadence turns KPIs into action rather than reporting artifacts.
Secure Staff Buy-In Through Involvement and Transparency
Frontline staff adopt new workflows when three conditions are met: they helped design them, they understand why the change was made, and they see evidence that it's working. Leadership that communicates improvement results visibly and regularly builds credibility for the next change cycle.
Workflows imposed top-down without frontline input tend to generate workarounds — the same informal processes that undermined the original workflow in the first place.
Staff buy-in is easier when teams can see the connection between their input and the outcome:
- Share before/after metrics with the units involved in pilots
- Name the staff members whose feedback shaped the final design
- Post results in common areas, not just leadership dashboards
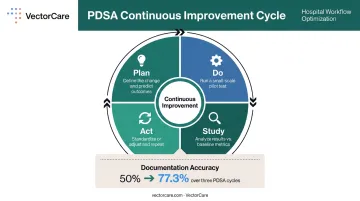
Pilot Before You Scale
Test workflow changes in one contained unit or process before organization-wide rollout. AHRQ's MATCH guidance recommends starting as small as one doctor, one nurse, or one patient. Most effective pilots run under a week and focus on confirming whether the change works as intended and identifying gaps that weren't visible in planning.
Iterative PDSA (Plan-Do-Study-Act) cycles applied consistently improve documentation accuracy and team confidence. One 2019 mixed-methods study found PDSA documentation accuracy improved from 50.0% to 77.3% over three rounds of structured support. The method itself compounds — teams get better at running cycles the more they run them.
Frequently Asked Questions
What is the workflow process in healthcare?
The healthcare workflow process is the structured sequence of tasks, decisions, and information handoffs that move a patient through care — from intake and assessment through treatment, discharge, and follow-up. It involves clinical staff, administrative teams, and technology systems working in coordination across multiple departments simultaneously.
What is an example of a workflow in a hospital?
Patient discharge is a clear example. A physician issues a discharge order, which triggers notifications to nursing, case management, pharmacy, and transport coordination — each completing their role in sequence so the patient leaves safely and the bed frees up for the next admission.
What are the most common bottlenecks in hospital workflows?
The most frequent sources of delay are poor handoff communication between departments, manual patient transport coordination, siloed EHR systems that don't share data in real time, and redundant documentation tasks that pull clinicians away from direct patient care.
How does patient transport and logistics affect hospital workflow?
Uncoordinated transport delays discharges, keeps beds occupied longer than necessary, and extends patient length of stay — all of which reduce care capacity and increase operational costs. Streamlining logistics coordination is one of the fastest ways to improve patient throughput without adding clinical resources.
How can hospitals measure whether their workflow improvements are working?
Key metrics to track include length of stay, discharge delays, door-to-physician time in the ED, transport wait times, and readmission rates. Baseline measurements captured before any changes give teams the data to evaluate true impact, not just anecdotal improvement.