According to AHRQ, 9 out of 10 hospitals have boarded admitted patients in the ED while waiting for inpatient beds — a figure that reflects systemic patient flow failure, not an ED-specific problem. Meanwhile, AHA data shows average hospital length of stay rose 19% between 2019 and 2022, with patients discharged to post-acute care seeing a 24% increase.
"Workflow improvement" sounds manageable. In practice, results vary enormously depending on where hospitals start, what they measure, and whether they treat logistics as infrastructure or a scheduling afterthought. This guide covers a concrete framework, the variables that determine success, and the mistakes that derail most efforts.
Key Takeaways
- Map existing workflows before changing them — document first, then fix
- Most bottlenecks are administrative, not clinical: communication gaps, discharge delays, and transport coordination top the list
- Technology only helps when it fits how care is actually delivered — mismatched tools create more work
- Patient logistics coordination is one of the highest-impact, most underinvested areas of workflow optimization
- Sustained improvement requires staff involvement, clear metrics, and continuous monitoring
A Step-by-Step Framework for Hospital Workflow Improvement
Workflow improvement happens in sequence. Skipping early steps tends to generate expensive rework.
Step 1: Map Your Current Workflows and Surface Hidden Bottlenecks
Start by documenting every step of key patient journeys — admission, diagnosis, treatment, discharge, and post-discharge handoff — as they actually happen, not as policy manuals describe them. AHRQ identifies Lean value stream mapping as a validated QI method for exactly this purpose, creating a visual map of each process step to expose handoffs, waiting time, and rework.
Involve frontline staff in mapping sessions. Nurses, transport coordinators, and admissions clerks carry the most consequential institutional knowledge — including the informal workarounds invisible to management, like nurses tracking transport by phone or staff maintaining shadow spreadsheets alongside the EHR.
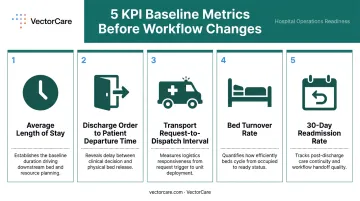
Before any changes are made, establish baselines on these KPIs:
- Average length of stay
- Time from discharge order to patient departure
- Transport request-to-dispatch interval
- Bed turnover rate
- 30-day readmission rate
Step 2: Standardize Clinical and Administrative Processes
Once bottlenecks are visible, define standard operating procedures for the highest-volume, highest-variance steps — patient admission protocols, triage criteria, medication order entry, and discharge checklists. The goal: outcomes should not depend on which individual is working that shift.
Standardization must be designed with clinical staff, not imposed on them. Research consistently shows that interdisciplinary input in workflow redesign is a key determinant of adoption.
Step 3: Modernize Communication Systems
Pagers and fax machines are not just outdated — they are measurably expensive. A peer-reviewed study found residents spent an estimated 67 minutes per 12-hour shift returning pages, with 68.3% of those pages nonurgent. A separate analysis found physicians, nurses, and pharmacists spent between 48 and 165 minutes per daytime shift on paging alone, at an estimated cost of $2,732 to $17,250 per month for a single medical ward.
Replacing these systems with secure, role-based digital messaging and real-time alerting reduces lag between clinical decisions and downstream actions — lab orders, pharmacy, transport, bed management. That lag is where patient wait times accumulate.
Step 4: Automate Patient Logistics and Transport Coordination
Patient logistics — ambulance transport, inter-facility transfers, NEMT, home health referrals, DME orders — is one of the most manual, phone-heavy segments of hospital operations. When it is treated as a scheduling afterthought rather than operational infrastructure, the result is extended length of stay, delayed discharges, and preventable readmissions.
A 2024 Joint Commission Journal study found that focused workflow intervention moved the median time from discharge order to patient departure from 3:23 p.m. to 2:27 p.m. — nearly a full hour earlier — while improving the share of discharges completed within 90 minutes of the discharge order from 26.2% to 38.1%.
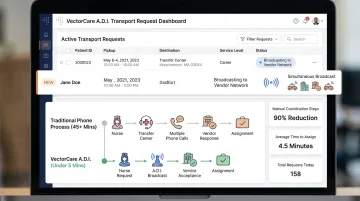
Automation platforms that integrate directly into EHR systems via SMART on FHIR can eliminate the manual broadcast-and-wait process. Instead of sequentially calling down a list, they broadcast requests simultaneously to all available providers. VectorCare's Automated Dispatching Intelligence (A.D.I.) addresses exactly this category of waste:
- Reduces transport request handling from 30+ minutes to under 3 minutes
- Drops to under 1 minute with full EHR integration
- Saved healthcare systems more than 100,000 hours in 2025 by eliminating phone calls, manual vendor negotiation, and data re-entry
Step 5: Integrate Systems to Eliminate Data Silos
Fragmented IT systems — separate EHRs, scheduling platforms, transport tools, and billing systems — are a leading cause of duplicated effort, missed information, and dangerous handoff errors.
According to ONC, 70% of U.S. hospitals engaged in all four domains of interoperable exchange in 2023, but only 43% did so routinely. That gap means the majority of hospitals still operate with partial or inconsistent data exchange.
Standards-based integration (HL7 FHIR, API-based connections) means a discharge note entered by a physician can automatically trigger logistics coordination, home health referrals, and DME ordering — without manual re-entry or additional phone calls.
When VectorCare's SMART on FHIR integration with Epic is active, patient demographics, insurance, encounter details, and clinical context are auto-populated into transport requests, removing an entire category of data entry and transcription error.
Step 6: Monitor Metrics Continuously and Sustain Gains Through Staff Engagement
Establish a small set of KPIs tied directly to workflow changes and review them on a regular cadence with both operational and clinical leadership:
- Bed turnover rate
- Discharge time (order to departure)
- Transport request-to-dispatch interval
- Avoidable readmission rate
Without a feedback loop, workflows drift back toward informal workarounds within months of a redesign. Sustainable improvement requires staff to understand why processes changed, see evidence that changes are working, and have a channel to report new friction points.
When Workflow Improvement Is Most Urgently Needed
Not every hospital needs the same intervention at the same time. Certain conditions signal that the cost of inaction is highest:
- ED boarding — admitted patients waiting hours for inpatient beds is a system-wide throughput failure
- Consistently high LOS relative to case-mix benchmarks
- Afternoon discharge clustering — most patients leaving after 3 p.m., limiting bed availability for new admissions
- High rates of transport-related complaints or missed transfer windows
Change events amplify every signal on that list. Hospitals undergoing EHR upgrades, mergers, or significant volume growth face the highest risk — informal processes that held together at lower volumes tend to break under new pressure. That's exactly when redesigning workflows matters more than digitizing existing workarounds.
Key Variables That Determine Workflow Improvement Outcomes
Two hospitals can follow the same framework and get very different results. Four variables explain most of the variance.
Information Handoff Quality
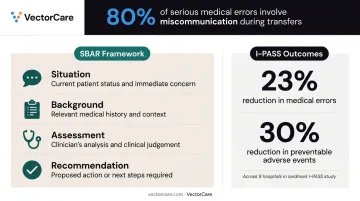
The Joint Commission estimates that 80% of serious medical errors involve miscommunication during patient transfers. AHRQ PSNet reports that an estimated 60% of medication errors occur during transitions of care.
Structured communication formats and digital tools directly address this risk:
- SBAR (Situation, Background, Assessment, Recommendation) gives clinicians a consistent framework for handoff conversations
- I-PASS, implemented across 9 hospitals, was associated with a 23% reduction in medical errors and a 30% reduction in preventable adverse events
- Digital handoff tools that carry forward relevant patient data automatically shorten the gap between clinical decision and next-step action, reducing the chance that critical information disappears between shifts
Patient Logistics Coordination
The time between a physician writing a discharge order and a patient physically leaving the hospital is one of the largest controllable drivers of length of stay. U.S. hospital stays exceeding three weeks account for 14% of all inpatient days and cost over $20 billion annually, with prolonged stays driven largely by non-clinical logistics delays.
Hospitals that automate logistics coordination and gain real-time transport visibility consistently report shorter LOS and faster bed turnover. VectorCare's hospital partners have documented over $500,000 in average annual savings per facility, driven by reductions in staff time spent on manual coordination, excess bed-days, and avoidable readmissions.
Technology Integration and Interoperability
A workflow tool that does not connect to the EHR becomes another system staff must manually reconcile, adding work rather than removing it. EHR-embedded applications — such as SMART on FHIR apps that surface logistics capabilities inside the clinical workflow — have higher adoption rates and produce more measurable workflow change than standalone applications requiring separate logins.
The practical result: fewer workarounds, faster task completion, and data that flows where it's needed without manual re-entry.
Staff Involvement and Change Management
Technology only holds if the people using it were part of shaping it. New tools and processes fail when staff weren't involved in the design phase or weren't adequately trained before go-live. Interdisciplinary involvement in workflow redesign — particularly from nurses and care coordinators who handle the highest volume of transition tasks — is one of the strongest predictors of successful implementation:
- Include frontline staff early in tool selection and process design
- Conduct structured training before go-live, not during it
- Build feedback loops so adoption gaps surface quickly after launch
Common Mistakes Hospitals Make When Improving Workflows
Workflow improvement projects fail in predictable ways. The four mistakes below account for most initiatives that stall, regress, or produce results that can't be measured.
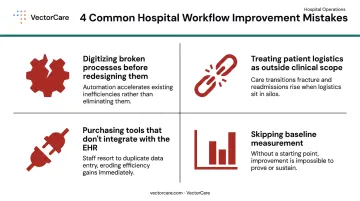
Digitizing broken processes before redesigning them. New technology applied to a dysfunctional process doesn't fix anything — it preserves the dysfunction in a shinier form. Automating phone tag rather than eliminating it, or digitizing a redundant approval step rather than removing it, produces the same delays with more complexity. Process mapping and redesign must come before technology selection, not after.
Treating patient logistics as outside clinical workflow scope. Many improvement initiatives focus on clinical and administrative processes while leaving transport coordination, inter-facility referrals, and discharge logistics to phone-based manual methods. That gap allows one of the largest drivers of extended length of stay and bed unavailability to persist, even after other improvements take hold.
Purchasing tools that don't integrate with the EHR. Standalone solutions that sit outside the EHR create new silos. Research consistently shows that poor EHR integration adds steps to clinical workflows rather than removing them. Any system that requires a separate login or manual data transfer will eventually be bypassed — not because staff are resistant to change, but because workarounds are faster.
Skipping the baseline measurement. Without pre-change data on specific operational KPIs, hospitals have no way to determine whether an intervention worked or justify continued investment. No baseline means no accountability, and no ability to distinguish genuine improvement from natural variation in daily volume.
Conclusion
Improving hospital patient workflows is a structured, iterative process. The hospitals achieving the most measurable gains are those that map first, redesign before digitizing, and treat patient logistics as core operational infrastructure rather than a back-office function.
The most durable improvements combine process standardization, modern communication tools, automated logistics coordination, and genuine staff engagement. Technology only delivers value when it fits the actual work — and platforms like VectorCare are built around that premise, automating the logistics layer so clinical teams can focus on care. Continuous monitoring is what turns a successful pilot into a permanent shift in how your hospital operates.
Frequently Asked Questions
What is an example of a workflow in healthcare?
The discharge workflow is a clear example: a physician writes the discharge order, a nurse prepares discharge instructions, transport is coordinated, home health or DME is arranged, and the bed is cleared for the next patient. A single unacknowledged transport request or unfilled DME order can bottleneck the entire chain.
What are the four types of workflows?
Healthcare workflows are typically categorized as inter-organizational (between facilities or providers), clinical-level (within a clinical practice or department), intra-visit (during a single patient encounter), and cognitive (the decision-making process guiding clinical judgment at each step). Intra-visit and inter-organizational workflows tend to surface the most visible delays and are where improvement efforts have the greatest impact.
What are the 5 P's of patient care?
The 5 P's — Pain, Position, Personal needs, Proximity to call light, and Plan of care — are a bedside rounding framework for proactively addressing patient needs before they become urgent. Checking these five items during scheduled rounds reduces unnecessary call lights and creates more predictable workflows throughout the shift.
What causes bottlenecks in hospital patient flow?
The primary causes include:
- Slow or fragmented discharge processes
- Manual transport and logistics coordination
- Siloed information systems that delay clinical decisions
- Communication gaps at shift changes and inter-departmental handoffs
Most bottlenecks are not clinical — they are administrative and logistical, which means they are also more directly addressable.
How does automating patient logistics reduce hospital length of stay?
When discharge transport, inter-facility transfers, and home health coordination are automated — replacing manual phone calls and fax-based requests — the time between a discharge decision and a patient physically leaving the hospital compresses significantly. That compression frees beds faster and eliminates avoidable overnight stays driven by logistics delays rather than clinical need.