Key Takeaways
- Healthcare meal delivery services range from inpatient hospital food systems to medically tailored meal (MTM) programs for patients managing chronic conditions at home.
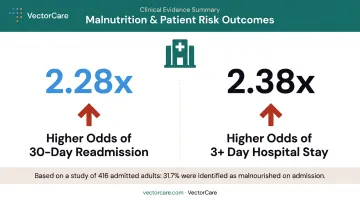
- Malnutrition is associated with 2.28x higher odds of 30-day readmission and 2.38x higher odds of longer hospital stays — making nutrition a measurable clinical risk factor, not a lifestyle concern.
- Traditional Medicare does not cover home-delivered meals — coverage falls to Medicare Advantage plans, Medicaid waivers, and state programs.
- Medically tailored meals differ from general meal kits by requiring dietitian oversight, clinical eligibility criteria, and alignment with therapeutic diets.
- Coordinating meal delivery alongside transportation, home health, and DME at discharge remains one of the most underdeveloped gaps in post-acute care.
What Counts as a Healthcare Meal Delivery Service?
The term "healthcare meal delivery" spans everything from hospital cafeteria trays to dietitian-prescribed home meals for kidney disease patients. The clinical stakes vary significantly depending on which layer of that spectrum a patient falls into.
A healthcare meal delivery service is any structured program that delivers nutritionally appropriate meals to patients — either within a clinical setting or at home as part of a care or recovery plan. Three distinct layers exist within that definition:
- Inpatient hospital food service — meals provided during an acute care stay, covered under Medicare Part A as part of inpatient hospital services
- Post-discharge or transitional meal programs — time-limited meal delivery triggered by a hospital discharge, often offered through Medicare Advantage supplemental benefits
- Community-based nutrition programs — long-term programs like Meals on Wheels or medically tailored meal (MTM) services for patients managing chronic conditions at home

What Makes a Meal "Medically Tailored"?
Of those three layers, medically tailored meals carry the most clinical weight — and the most precise definition. According to HHS ODPHP, MTMs are fully prepared meals provided to patients with complex medical conditions who cannot shop or cook. The Academy of Nutrition and Dietetics identifies registered dietitian nutritionists (RDNs) as essential to any rigorous food-as-medicine program.
That means each MTM is prescribed or dietitian-designed for a specific diagnosis:
- Renal diets for kidney disease
- Cardiac or low-sodium meals for heart failure
- Carbohydrate-controlled meals for diabetes
- High-protein meals for oncology patients
- Texture-modified meals for those with dysphagia
A commercial meal kit is built around culinary variety and convenience. An MTM is built around a diagnosis. That distinction matters when evaluating whether a program qualifies for clinical reimbursement or care plan integration.
Who Uses These Services?
- Elderly patients, especially those who are homebound or have limited mobility
- Patients with chronic conditions — diabetes, heart disease, COPD, renal disease, cancer
- Post-surgical recovery patients requiring specific nutrient support
- Food-insecure individuals for whom discharge planning otherwise fails
- Patients transitioning from skilled nursing facilities or hospitals to home settings
Types of Healthcare Meal Delivery Programs
Inpatient Hospital Meal Systems
During an acute inpatient stay, meal delivery is part of the hospital's food service operation. Medicare Part A covers meals as a standard component of inpatient hospital services. These systems typically include therapeutic diet menus, patient-specific tray assembly, and temperature-controlled delivery. The operational focus is safety and clinical compliance — allergen management, texture modification, and diet restriction accuracy are managed centrally.
The limitation is inherent: inpatient meals end at discharge. Whatever nutritional needs drove the admission continue at home, where no equivalent system automatically exists.
Medically Tailored Meal (MTM) Programs
Medically Tailored Meal (MTM) programs are community-based interventions where meals are designed by registered dietitians for patients with serious illnesses. Unlike hospital food service, MTMs are delivered to a patient's home over weeks or months and are tied to a clinical diagnosis and care plan.
The federal policy pathway gaining the most traction is CMS's Medicaid Health-Related Social Needs (HRSN) framework. It allows certain nutrition supports — including home-delivered meals — under Section 1115 demonstrations for up to 3 meals per day for up to 6 months. That makes it the strongest federal mechanism currently available for MTM-scale benefits in Medicaid populations.
Meals on Wheels and OAA Nutrition Programs
The Older Americans Act (OAA) Title III-C nutrition program funds both congregate and home-delivered meals for adults 60 and older. It operates through a tiered network:
- 56 State Units on Aging
- 600+ Area Agencies on Aging
- More than 5,000 local providers
Meals must provide at least one-third of Dietary Reference Intakes.
OAA meals serve a different purpose than MTM programs. They are a senior nutrition and social support benefit — not a disease-specific clinical intervention — though they provide meaningful nutritional support and often include wellness checks that catch early health deterioration.
Medicare Advantage Supplemental Meal Benefits
Some Medicare Advantage plans offer supplemental meal delivery as a post-hospitalization benefit. A 2023 cohort study examined a 4-week post-hospitalization MA meal benefit and found it associated with lower 30-day death or rehospitalization — with heart failure patients showing 23.3% unadjusted 30-day death or rehospitalization compared to 38.5% among those not reached or declining the benefit.
These benefits are plan-specific: duration, eligibility trigger, and member criteria vary. Care teams should verify coverage directly in each plan's Evidence of Coverage document before assuming this benefit is available.
State Medicaid Programs Worth Knowing
Three state examples illustrate how Medicaid meal benefits are structured at the state level:
- California CalAIM: Medically tailored meals are an available Community Support within managed care plans, though plan election and member criteria vary
- North Carolina Healthy Opportunities Pilots: The nation's first comprehensive Medicaid program testing evidence-based non-medical interventions, including nutrition supports, for high-needs members in pilot regions
- Colorado HCBS: Home-delivered meals are available to eligible waiver members discharged from the hospital or transitioning into the community
How Healthcare Meal Delivery Improves Patient Outcomes
The clinical case for these programs isn't speculative. The evidence is specific enough to shape discharge planning priorities.
Malnutrition Drives Readmissions and Longer Stays
A 2022 cohort study of 416 adults admitted in Houston found that 31.7% were malnourished on admission. Malnutrition was associated with 2.28x higher odds of 30-day readmission and 2.38x higher odds of a length of stay of three or more days. These are not marginal differences.
A separate national inpatient sample analysis found diagnosis-coded malnutrition rose from 6.6% to 8.6% across more than 66 million US hospitalizations between 2016 and 2019. The direction of the trend matters: malnutrition risk in hospitalized patients is increasing, not decreasing.
Nutrition Supports Wound Healing and Recovery
The clinical mechanism is straightforward. Adequate protein and key micronutrients (vitamins A, B, and C, zinc, omega-3 fatty acids, and specific amino acids) directly support wound healing and immune function. Malnutrition impairs all of these, extending recovery timelines and increasing susceptibility to complications.
For post-surgical patients and those recovering from pressure injuries, this is not a secondary concern. It's a primary driver of how quickly a patient can safely return home.
Food Insecurity Breaks the Rest of the Care Plan
For food-insecure patients, the gap is more fundamental. Research has found prescription medication nonadherence is associated with food insecurity — patients who cannot afford food also skip medications. Discharge planning that addresses transportation, follow-up appointments, and medication management fails when the patient cannot access appropriate food at home.
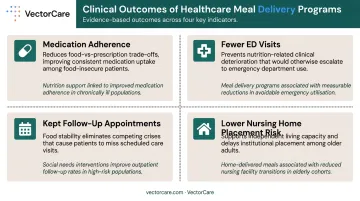
Meal delivery closes that gap directly. When included in the discharge plan, it supports:
- Medication adherence, since patients are no longer trading food costs against prescriptions
- Fewer emergency department visits tied to nutrition-related deterioration
- Higher rates of kept follow-up appointments, as food stability reduces competing crises
Supporting Independent Living and Reducing Nursing Home Placement
A 2023 pragmatic randomized trial of 243 homebound adults 66 and older with dementia found that daily home-delivered meals showed a lower (though not statistically significant) likelihood of nursing home placement at six months compared to drop-shipped meals. The evidence is promising, not definitive — but the direction aligns with what independent living research consistently shows: reducing nutritional instability lowers institutionalization risk for high-acuity patients.
What to Look for When Evaluating a Healthcare Meal Delivery Service
Not all meal delivery services are built for clinical settings. Three areas separate vendors that can support real care programs from those better suited to general consumer use.
Therapeutic Diet Compliance and Dietitian Oversight
- Confirm a registered dietitian is involved in menu development, not just general nutrition guidelines
- Ask whether meals are reviewed for specific clinical conditions: renal, cardiac, diabetic, oncology, texture-modified
- Check whether patient-level customization is available — allergen exclusions, texture modification, cultural preferences
- Determine whether ordering can connect to discharge orders or care plan documentation
Delivery Reliability and Cold Chain Management
- Evaluate how meals are maintained at safe temperatures during transit
- Clarify delivery frequency and what happens when a patient is unavailable at the time of delivery
- Confirm the provider has a process for missed deliveries and schedule changes
Accreditation, Credentialing, and HIPAA Compliance
For healthcare facilities procuring meal delivery as part of a care program, compliance requirements add another layer of vendor evaluation:
- Confirm the provider holds relevant accreditations or has been vetted through a clinical procurement process
- Verify that data sharing related to patient dietary needs complies with HIPAA
- Determine whether the provider can participate in payer billing or reimbursement workflows where applicable
Coverage and Funding for Healthcare Meal Delivery
Does Medicare Cover Meal Delivery?
Traditional Medicare (Parts A and B) does not cover home-delivered meals. Medicare Part A covers hospital meals during inpatient stays, and Medicare's home health coverage explicitly excludes home meal delivery. This is a common source of confusion at discharge.
Some Medicare Advantage (Part C) plans add supplemental meal delivery benefits — typically triggered by hospitalization and limited to a defined number of weeks. Coverage windows, eligibility criteria, and meal quantities are plan-specific.
Medicaid and State Waiver Programs
Medicaid coverage varies significantly by state. Key pathways:
- Section 1115 HRSN demonstrations: Allow home-delivered meals or pantry stocking for up to 3 meals per day for up to 6 months for eligible members
- 1915(c) HCBS waivers: Some states include home-delivered meals as a waiver service for members transitioning from institutional to community settings
- Medicaid managed care in-lieu-of services: Plans may offer meals as an alternative to higher-cost services
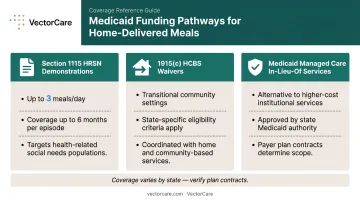
Care teams should check their state's specific waiver structure and managed care plan contracts — there is no uniform national benefit to assume. Even thorough Medicaid verification will leave some patients without a covered pathway, which is where other funding sources become essential.
Other Funding Pathways
For patients who fall outside Medicare and Medicaid eligibility, several additional sources can fill the gap:
- Older Americans Act / Area Agencies on Aging — for adults 60+ with economic or social need
- USDA nutrition programs — SNAP and other food assistance
- Nonprofit and foundation grants — many community food organizations have restricted funding for specific patient populations
- Health system community benefit funds — hospitals that must demonstrate community benefit can sometimes fund meal programs directly
A care coordinator may need to assemble a patchwork of these sources for a single patient — and doing so can mean navigating three or four separate applications, eligibility checks, and funding timelines simultaneously. That overhead rarely appears in discharge planning workflows, even though it directly affects whether patients eat consistently after leaving the hospital.
Coordinating Healthcare Meal Delivery: The Operational Challenge
The clinical evidence for meal delivery programs is increasingly solid. The operational infrastructure to deliver on that evidence is not.
Discharge planners currently manage meal referrals through the same fragmented workflows that complicate every other post-discharge service: phone calls to meal providers, manual eligibility checks, paper or fax-based referrals, and no systematic tracking of whether meals were actually delivered and consumed.
These tasks sit outside the EHR, outside home health scheduling systems, and outside payer authorization workflows.
The consequence is predictable. A 2021 retrospective cohort study of 50,772 adults found 30-day readmission was 6.0% among patients who made their follow-up appointment versus 8.8% among those without follow-up. Meal referrals face the same completion gap as follow-up appointments, and receive far less systematic tracking.
What Unified Coordination Infrastructure Changes
Platforms like VectorCare, which are built to unify non-emergency patient logistics across a connected provider network, represent the infrastructure layer that healthcare facilities need to coordinate post-discharge services — including transportation, home health, and DME — without the fragmentation that creates care gaps.
When multiple post-discharge services are managed through a single coordinated system rather than separate manual workflows, the practical result is measurable:
- Fewer missed handoffs between discharge planners and service providers
- Real-time visibility into whether services were actually fulfilled
- Faster escalation when a meal delivery or follow-up falls through

Discharge coordinators can track whether services were completed rather than assuming they were. That visibility is what converts a good discharge plan into a completed one.
VectorCare's platform currently supports this coordination model across transportation, home health, and DME within a single interoperable system, with SMART on FHIR integration that embeds logistics coordination directly into existing clinical workflows rather than alongside them.
Frequently Asked Questions
Does Medicare cover meal delivery?
Traditional Medicare does not cover home-delivered meals. Medicare Part A covers meals during an inpatient hospital stay. Some Medicare Advantage plans offer supplemental meal benefits post-hospitalization, but coverage duration and eligibility criteria vary by plan — check the specific plan's Evidence of Coverage.
What is the best meal delivery system for healthcare settings?
It depends on the care setting. Inpatient settings need temperature-controlled tray delivery with dietary restriction management. For community-based programs, the priorities are dietitian oversight, therapeutic diet alignment, reliable last-mile delivery, and integration with discharge planning workflows.
What is a medically tailored meal?
A medically tailored meal is a fully prepared meal designed by a registered dietitian for a patient with a specific medical condition — such as renal disease, heart failure, or diabetes. MTMs meet clinical nutrition targets specific to that condition, not just general healthy eating guidelines.
Who qualifies for healthcare meal delivery services?
Eligibility depends on the program and funding source. Inpatient patients receive meals as part of their stay. Community-based programs typically serve seniors, people with chronic conditions, post-surgical patients, or food-insecure individuals — with funded programs through Medicare Advantage, Medicaid, or OAA varying by payer and state.
How do healthcare meal delivery services differ from regular meal kit services?
Healthcare meal delivery programs require clinical eligibility, dietitian oversight, and therapeutic diet compliance. They are often subsidized through insurance or government funding. Commercial meal kits are designed for culinary variety and convenience — not clinical nutrition management.
Can healthcare meal delivery reduce hospital readmissions?
Clinical evidence supports a connection between consistent, medically appropriate nutrition post-discharge and lower readmission rates. A Medicare Advantage cohort study found that a 4-week post-hospitalization meal benefit was associated with significantly lower 30-day death or rehospitalization in heart failure patients. While the relationship is associative rather than causal, findings point in the same direction across multiple independent studies.