Introduction
A mid-sized hospital coordinates hundreds of moving parts every day — beds, staff rotations, operating rooms, referral queues, discharge transports, equipment deliveries. Most hospitals have invested in EHRs, scheduling portals, and calendar software. Yet the coordination burden hasn't meaningfully shrunk. Digitizing records didn't fix the underlying process — it just moved the friction online.
According to ONC data, hospital use of EHR-integrated predictive AI for scheduling rose from 51% to 67% between 2023 and 2024. That growth signals a real shift — but deployment remains uneven. Automated visit scheduling is fully deployed in just 2% of surveyed health systems, while census and staffing forecasting reaches only 21%.
Most hospitals are still operating in that gap — running automated reports while coordinating transport, staffing, and discharges by phone. This guide breaks down how AI actually works across appointment booking, staffing, OR coordination, referral routing, and the patient logistics layer that most scheduling tools don't touch.
Key Takeaways
- AI hospital scheduling automates constraint matching across providers, rooms, equipment, and insurance — not just calendar management
- Deployment varies sharply: OR optimization is fully live in 14% of health systems; automated visit scheduling in just 2%
- Referral loop closure sits below 35% in many health systems — a gap AI routing directly addresses
- Patient logistics (transport, discharge, home health) remains the most underserved automation layer
- HIPAA compliance and human oversight are baseline requirements for any clinical scheduling AI deployment
What AI Hospital Scheduling Automation Actually Is
AI hospital scheduling automation uses machine learning and intelligent agents to manage and coordinate the scheduling of patients, staff, and clinical resources — without requiring manual input for routine decisions. Hospital operations involve hundreds of interdependent variables at once:
- Provider availability and credentialing
- Insurance eligibility and prior authorization status
- Room, equipment, and bed capacity
- Staff-to-patient ratios and shift coverage
- Urgency levels and clinical sequencing requirements
Manual coordination cannot sustain that complexity at scale. When MGMA tracked the impact of online appointment scheduling, they found a 4.1% decrease in inbound call volume and a 5.2% decrease in employee phone time — even from basic digitization alone. AI goes further by processing constraints dynamically and executing multi-step decisions without a coordinator in the loop.
What distinguishes AI scheduling from legacy software:
- Legacy tools store templates and flag conflicts — humans resolve them
- AI systems predict demand, match constraints in real time, and execute decisions for routine cases without waiting for a coordinator
- Patterns like no-show history, volume trends, and cancellation rates feed back into the system, improving future decisions automatically
The result is a coordination layer that handles the cross-referencing a scheduler would otherwise do manually — across multiple systems, simultaneously, at scale.
How AI Automates the Scheduling Workflow
AI-driven scheduling operates in defined stages — from request capture through confirmation and downstream integration. Each stage reduces the manual effort that previously slowed the process.
Initiation: Capturing the Request
Patients, providers, or systems can trigger a scheduling request across multiple channels — phone, patient portal, text message, or EHR referral submission. AI systems receive and interpret these inputs using natural language processing (NLP) to extract intent, urgency signals, and relevant patient details.
Initiation doesn't always require a person. Prior authorization approval can automatically launch a scheduling workflow. A referral order submission can trigger patient outreach before anyone manually reviews it — the AI doesn't wait for a coordinator to begin.
Core Processing: Matching Demand to Availability
Once a request is captured, the AI simultaneously checks:
- Real-time provider availability
- Appointment duration requirements
- Insurance eligibility
- Room or equipment needs
- Practice-specific scheduling rules
This constraint matching replaces what a human coordinator would do by manually cross-referencing three to five separate systems. Direct EHR integration via standards like SMART on FHIR writes confirmed appointments back into provider calendars instantly, eliminating transcription errors.
Optimization: Filling Gaps Before They Cost You
Static scheduling creates revenue gaps every time a cancellation goes unaddressed.
When a slot opens, the system immediately cross-references the waitlist against clinical urgency, patient proximity, and provider preference — and fills the gap automatically. Predictive capabilities add another layer: patients flagged as likely to no-show (based on historical patterns) receive proactive outreach before the gap occurs.
One peer-reviewed study at a 600-bed university hospital reported $20,610 in revenue recaptured in a single pilot month from AI-based no-show management alone.
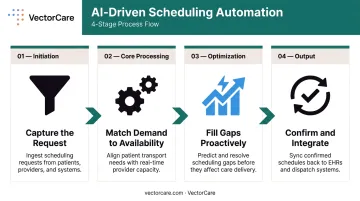
Output: Confirmed Scheduling and Downstream Integration
The automation produces a confirmed, rule-compliant appointment that flows directly into:
- EHR systems and provider workflows
- Pre-visit intake sequences
- Reminder and authorization tracking
- Any downstream operational systems
Every step — from initial request to downstream system updates — completes without a coordinator touching the record.
Key Hospital Operations AI Is Transforming
Appointment scheduling is one node in a much larger operational network. AI is being applied across staffing, clinical resource management, and patient flow — with measurable results in each area.
Bed Management and Patient Flow
AI-powered bed management tools provide real-time census data and predictive capacity forecasting. Nurse managers and operations teams can anticipate demand before it hits, reducing boarding time and improving throughput — not scrambling to respond once capacity is already strained.
Cleveland Clinic's Hospital 360 Virtual Command Center is one of the clearest real-world examples: it provides real-time patient census, capacity forecasts, transfer volume tracking, and time-to-bed-assignment tracking — all in a single operational view.
Nurse Staffing and Shift Optimization
AI staffing tools align nurse-to-patient ratios with actual predicted demand rather than static historical models. Cleveland Clinic's Staffing Matrix, for instance, uses real-time volume prediction to give nurse managers shift-level and week-level projections — including scheduled RNs, call-offs, and float pool availability.
Across surveyed health systems, **21% have fully deployed AI for census and staffing forecasting**, with another 48% developing or piloting it — the highest adoption rate of any scheduling AI category.
OR Scheduling and Surgical Resource Optimization
OR scheduling requires pulling together provider availability, equipment requirements, room scheduling, and PACU capacity simultaneously. AI systems identify optimal surgical sequencing and flag utilization gaps. The reactive model — spreadsheets, sticky notes, manual block reviews — gets replaced with evidence-based forecasting.
Cleveland Clinic's OR Stewardship module provides real-time scheduling opportunities, case-prediction analyses, and PACU capacity estimates. A 2024 systematic review confirmed AI and ML are producing measurable gains in surgical duration prediction and OR resource management across multiple health system settings.
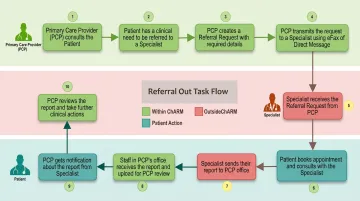
Referral Routing and Intake Automation
The referral process is one of the most broken workflows in healthcare. A large academic health system study found documented referral-loop closure was under 35% — meaning most referrals simply don't result in a confirmed appointment.
AI handles referral intake by automatically determining the appropriate specialist based on clinical need and insurance network, then reaching out to the patient and booking the appointment. A multi-day manual process compresses to minutes. Every unconfirmed referral is a patient who didn't receive care and revenue that didn't reach the system.
Pre-Visit Coordination and Access Center Workload
After booking, AI automates the pre-visit sequence:
- Intake form delivery and collection
- Insurance verification
- Authorization flagging
- Reminder sequencing
On the access center side, AI distributes inbound workload by complexity and urgency — routing simple requests to automated resolution and escalating complex cases to coordinators. This reduces cognitive overload and improves resolution speed without adding headcount.
Patient Logistics: The Layer Most AI Scheduling Tools Miss
Most AI scheduling platforms stop at the appointment. What happens after — how the patient physically moves through and between care settings — is treated as someone else's problem.
It shouldn't be.
What Patient Logistics Actually Covers
Patient logistics is the full coordination chain that determines care continuity:
- Non-emergency medical transport (NEMT) to and from appointments
- Discharge transport coordination
- Post-acute and home health scheduling
- Durable medical equipment (DME) delivery
- Interfacility and air medical transfers
Nearly 30% of older individuals experience hospital discharge delays — and when transport isn't confirmed, patients sit in beds that should be turning over. Medicaid NEMT alone represents $2.6 billion in annual spending, confirming the operational scale of this coordination layer.
Why Standard AI Scheduling Tools Fail Here
Standard scheduling tools are built for appointment booking within a single facility or EHR system. They lack:
- Multi-party coordination logic across independent transport networks
- Real-time provider broadcasting and response handling
- In-transit tracking across different transport modalities
- Rate negotiation and billing integration across external vendors
Coordinating a discharge transport requires broadcasting to a provider network, managing responses, confirming the assignment, and tracking execution to completion. Scheduling software isn't built for that. It's a logistics infrastructure problem.
How Automated Dispatching Addresses the Gap
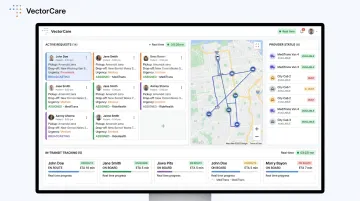
Platforms built specifically for patient logistics replace the phone-based dispatch model with automated network broadcasting. When a hospital needs to arrange non-emergency transport or coordinate a post-discharge transfer, the system broadcasts the request to qualified providers, manages responses, confirms the assignment, and tracks the task to completion with no manual phone calls required.
VectorCare's A.D.I. (Automated Dispatching Intelligence) operates at this scale — processing a new request every 23 seconds, sending broadcasts every 12 seconds, and saving healthcare systems more than 100,000 hours across patient logistics workflows in 2025.
The results are measurable at the facility level too. One documented case study showed transport request time dropping from 45 minutes to 4.5 minutes after implementation.
The downstream effects extend beyond time savings:
- Shorter patient length of stay
- Reduced bed holds from discharge delays
- Fewer gaps in post-acute care transitions
- Improved coordination between hospitals, transport providers, home health agencies, and DME suppliers
VectorCare's SMART on FHIR integration with Epic means the entire workflow — from discharge order to transport confirmation — initiates directly from within the EHR, with patient data pre-populated automatically. No manual transcription, no parallel phone calls.
Where AI Scheduling Has Real Limits
AI scheduling performs well when decisions are rule-based, structured, and involve clearly defined parameters. It creates risk when applied to scenarios requiring clinical judgment.
Areas where human oversight is non-negotiable:
- Emergency triage and symptom-driven urgency classification
- Complex multi-provider sequencing where visit order depends on clinical findings
- Psychiatric crisis routing
- Any case where the "right" answer requires contextual reasoning beyond the defined ruleset
The appropriate model is supervised automation: humans define the rules and handle edge cases; AI applies those rules consistently at scale and escalates unclear or high-risk requests to clinical staff. The division is deliberate — AI handles volume and consistency, while clinical staff retain authority over judgment calls.
Any AI system handling protected health information (PHI) in a scheduling context must meet the HIPAA Security Rule's requirements for administrative, physical, and technical safeguards. That includes access control, audit controls, integrity verification, person/entity authentication, and transmission security.
AI vendors who create, receive, maintain, or transmit ePHI on behalf of a covered entity are business associates and require written BAAs — regardless of whether the vendor can view the encrypted data.
HIPAA compliance is a baseline product requirement. Vendors who present it as a selling point are describing table stakes.
Frequently Asked Questions
What types of hospital operations can AI automate beyond appointment scheduling?
AI is actively automating across several distinct operational areas:
- Staffing optimization and shift management
- Bed management and patient flow
- OR scheduling and surgical resource coordination
- Referral routing and intake
- Pre-visit coordination
- Patient transport and discharge logistics
How does AI in hospital scheduling integrate with existing EHR systems?
Most platforms use SMART on FHIR standards — specifically the HL7 SMART App Launch framework — which allows AI systems to read real-time availability and write confirmed appointments or updates back into the EHR without manual data entry. Epic, the most widely used hospital EHR, supports this standard directly.
Is AI-driven hospital scheduling HIPAA compliant?
Compliant systems use encrypted, HIPAA-secure infrastructure with access controls, audit trails, and transmission security. Any vendor handling ePHI must sign a Business Associate Agreement (BAA). BAA verification is a required step before any production deployment, not something to confirm after go-live.
How long does it take to implement AI scheduling automation in a hospital?
Timelines vary by system complexity and EHR integration requirements. Platforms with pre-built EHR connectors and SMART on FHIR certification typically go live in weeks rather than months. Custom-built integrations take longer — often several months depending on scope and IT resource availability.
What is the ROI of AI automation for hospital scheduling and operations?
Measurable outcomes include reduced no-show rates, staff hours recovered, revenue recaptured from filled slots, and lower administrative labor costs. One peer-reviewed study at a 600-bed university hospital reported $20,610 in pilot-month revenue from AI-based no-show management. On the logistics side, a large California payer-provider saved $22 million annually after deploying automated dispatching for post-discharge coordination.
Can AI handle patient transport and discharge coordination, not just appointment booking?
Yes — automated dispatching platforms extend AI into the patient logistics layer by coordinating NEMT, discharge transport, home health scheduling, and interfacility transfers. These systems broadcast requests to provider networks, confirm assignments, and track tasks through to completion.