Introduction
Hospital scheduling is not just about booking time slots. It's the coordination layer that determines whether patients actually receive care — and right now, that layer is buckling under pressure.
Inpatient volumes rose 5.3% and outpatient visits climbed 9.8% in 2025, according to the American Hospital Association. Meanwhile, hospitals spent over $1 trillion on workforce costs that same year, with administrative and billing staff alone accounting for 6.5% of total hospital employment. The math doesn't work with manual processes.
AI-driven scheduling automation is filling this gap — not as a future-state ambition, but as an operational reality hospitals are deploying today. The five applications below cover where AI is already cutting wait times, reducing no-shows, and moving patients through the system faster — from initial access to post-discharge coordination.
Key Takeaways
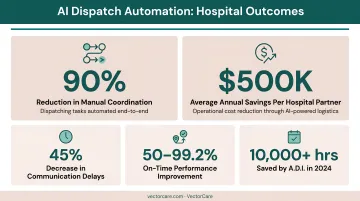
- AI dispatch systems like VectorCare's A.D.I. are cutting manual transport coordination by 90%, saving hospital partners $500K+ annually
- 89% of patients say anytime digital scheduling is important, yet most health systems still lack the tools to deliver it
- Automated reminders cut no-show rates from 24% to 14% in peer-reviewed trials, protecting significant revenue
- SMART on FHIR integration with Epic cuts scheduling time from 31 minutes to under one minute by eliminating manual re-entry
- Running post-acute care coordination in parallel rather than sequentially cuts length of stay and lowers readmission risk
Way 1: Automated Dispatching Intelligence for Transport Scheduling
The Manual Dispatch Problem
When a patient needs transport, the traditional workflow looks like this: a case manager calls a list of providers, waits for callbacks, re-enters patient information, confirms logistics, and follows up again. For a 250-bed hospital handling 25 daily transports, that manual cycle consumes roughly 4,714 staff hours per year — about 31 minutes per request.
That's not a staffing inconvenience. It's a structural bottleneck that delays discharges, ties up beds, and keeps nurses on hold instead of at the bedside.
How A.D.I. Changes the Equation
VectorCare's Automated Dispatching Intelligence (A.D.I.) replaces that phone-tag cycle. The system simultaneously broadcasts transport requests to the appropriate network of NEMT, ground ambulance, and air medical providers — matching them based on:
- Patient acuity and level of service (BLS, ALS, CCT, SCT)
- Geographic service zones and real-time availability
- Credential and policy compliance via automated vendor verification
- Cost optimization rules (lowest cost, fastest ETA, or custom blended policies)
In 2024, A.D.I. processed over 2.3 million broadcasts with contract value exceeding $570 million, saving customers over 10,000 hours in coordination labor. By 2025, that figure grew to more than 100,000 hours saved across the platform.
Documented Hospital Outcomes
Hospital partners implementing A.D.I. report consistent results:
- 90% reduction in manual coordination tasks
- 45% decrease in communication-related delays
- $500,000+ in average annual savings at larger facilities
- $247,000 in bed-throughput savings at hospitals under 250 beds
One of California's largest healthcare providers saved $22 million annually after implementing VectorCare in 2019, reducing per-request scheduling time from 30 minutes to under 5 minutes. Orange County Health Care Agency achieved a 10x reduction in transport arrangement time, dropping from 45 minutes to 4.5 minutes per request.
As health systems decentralize care and interfacility transfer volumes grow, sequential phone-based dispatch cannot keep pace. The facilities posting these results aren't outliers — they're the early movers in a shift that's now reaching every tier of the hospital market.
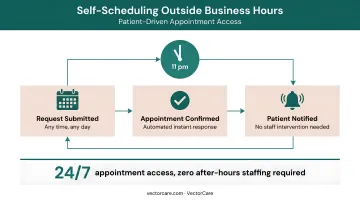
Way 2: 24/7 AI-Powered Appointment Booking and Self-Service Patient Access
Patient expectations have shifted faster than most health systems have adapted. According to MGMA's 2024 data, 89% of patients say anytime digital appointment scheduling is important — yet 73% of medical group leaders report that 25% or fewer of their patients actually use digital tools to schedule. Only 11% of leaders say a majority of patients self-schedule.
That gap between demand and delivery costs health systems patients, staff time, and revenue.
What AI Scheduling Actually Enables
Platforms with natural language understanding let patients describe their needs in plain terms. The system interprets clinical context and routes them to the correct appointment type without staff involvement — reducing misrouted bookings and unnecessary escalations.
Key operational benefits include:
- Processes requests around the clock, including overnight and weekends when no staff is available
- Cuts inbound call volume for routine bookings, freeing staff to handle complex cases
- Reduces scheduling errors by capturing data directly from patients rather than through phone transcription
A peer-reviewed scoping review found that 34% to 51% of self-scheduled appointments occur outside regular office hours — time when no staff member would have answered a phone. That's new access capacity created without adding headcount.
Healthgrades' 2025 survey found 55% of respondents would consider switching providers for one offering online scheduling. Scheduling friction is both an operations problem and a competitive one.
VectorCare's DispatchCare portal extends this same self-service logic to patient logistics: patients, family members, and caregivers can book transport, DME delivery, and ancillary services directly from a phone or browser, any time, with real-time ETAs and automated status notifications.
Way 3: Predictive No-Show Reduction and Intelligent Waitlist Management
Missed appointments cost the U.S. healthcare system more than $150 billion per year, according to a peer-reviewed oncology access study. For individual specialties, a 2023 radiation oncology study found 9% of scheduled patients failed to show, with nearly half of those no-shows occurring without any prior notice.
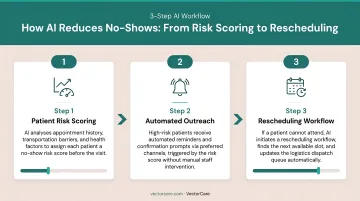
How AI Reduces No-Show Rates
The clinical evidence for automated reminders is solid. A JAMA-published trial found reminder interventions reduced no-show rates from 24% in control groups to 14% — a 10-percentage-point reduction from a single intervention layer. Add personalized, multi-channel outreach calibrated to individual patient communication preferences and no-show rates drop further still.
AI-driven no-show reduction works by:
- Scoring each patient's no-show risk using appointment type, lead time, attendance history, and demographic signals
- Sending reminders via SMS, email, or voice at intervals calibrated to each patient's communication profile
- Offering one-tap rescheduling so patients who can't attend convert to a filled slot instead of a missed one
VectorCare's platform includes SMS Patient Reminders & Cancellations as a core capability, automating the communication loop between patients, providers, and transport services — particularly for patients with recurring chronic care appointments who need regular transport coordination.
Intelligent Slot Recovery
Reminders reduce no-shows significantly, but cancellations still happen. When they do, the cost isn't just lost revenue — it's wasted clinical capacity that's nearly impossible to recover manually. Intelligent waitlist automation scans the cancellation against eligible waitlisted patients based on clinical priority, provider availability, and insurance status, then sends outreach automatically. No staff involvement, no manual list-checking.
For high-demand specialties where waitlists stretch weeks out, that automated recovery can mean earlier care for a patient who needed it — and a schedule that runs at full clinical capacity instead of absorbing the revenue loss quietly.
Way 4: EHR Integration and Automated Patient Data Extraction for Scheduling
Manual data entry between scheduling systems and EHRs is one of the most persistent inefficiency sources in hospital operations. Every time a care coordinator re-enters patient demographics, insurance information, or clinical details into a separate system, there's an opportunity for error. The Joint Commission reports that nearly 67% of medical errors stem from handoff breakdowns.
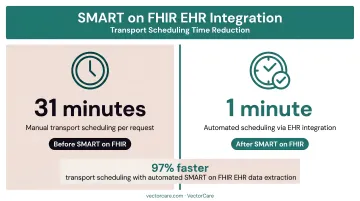
What SMART on FHIR Enables
ONC data shows that 96% of non-federal acute care hospitals now hold a certified EHR, and hospital use of FHIR-based APIs for patient app access grew from 62% in 2021 to 74% in 2022. The infrastructure for real-time, bidirectional EHR integration now exists at scale — it didn't five years ago.
VectorCare's SMART on FHIR app for Epic pulls the following data automatically when a transport or scheduling request is initiated:
- Patient demographics, MRN, and insurance coverage
- Encounter details, admission/discharge dates, and current location
- Vital signs, conditions, isolation status, and ventilator requirements
- IV drip details, weight, and bariatric considerations
- Attending physician information
This eliminates the need for coordinators to toggle between systems. The result: scheduling time drops from approximately 31 minutes per transport to under one minute. For a 250-bed hospital, that's the difference between 4,714 coordination hours per year and 456.
Priority Dispatch Corp Partnership
VectorCare's partnership with Priority Dispatch Corp extends this automation to full interfacility transfer workflows. Their Medical Transfer Protocol (MTP) SMART on FHIR app — launched in the Epic Showroom in April 2026 — lets transfer center coordinators initiate and manage transfers without leaving Epic.
The app covers three transfer types, each with ICD-10 billing codes attached at the dispatch level:
- Protocol 45: Unscheduled up-care transports
- Protocol 46: Routine scheduled transfers
- Protocol 47: Mental health transfers
Triage details auto-document directly in the patient chart, cutting follow-up calls and reducing billing department workload at the same time.
Epic is the most common entry point, but the same bidirectional data exchange extends across other major platforms. VectorCare Connect supports Cerner, Meditech, Athenahealth, and additional EHRs through HL7 v2 messaging and FHIR R4 APIs.
Way 5: AI-Driven Care Coordination Across Post-Acute Service Levels
Discharge planning is where hospital scheduling meets real financial consequence. When post-acute services — transport, DME, home health, pharmacy, SNF placement — are coordinated sequentially after discharge orders are written, delays cascade. Beds stay occupied. ED throughput backs up. And patients get home without the services they need to stay home.
AHRQ data puts the average 30-day all-cause readmission cost at $16,300 — 12.4% higher than the average index admission. Under the Hospital Readmissions Reduction Program, CMS can cut Medicare payments by up to 3% for excess readmissions. With 44.9% of U.S. healthcare payments now flowing through alternative payment model contracts that include downside risk, readmissions have direct financial consequences for most major health systems.
Parallel Coordination vs. Sequential Coordination
VectorCare's Post-Discharge Home Care Coordination module fires a unified workflow directly from Epic at the moment of discharge. Rather than sequencing each service request, the platform coordinates simultaneously:
- Transport home matched to the appropriate modality (NEMT, wheelchair van, stretcher, rideshare)
- DME delivery and setup routed to contracted providers with full clinical context, tracked through completion
- First home health visit scheduled within the Start of Care (SOC) window, with intake integration
- SNF or rehab placement with real-time bed availability search and interfacility transfer coordination
- Pharmacy and meal delivery where applicable
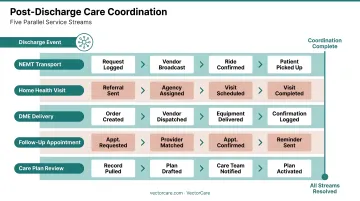
Case managers get real-time visibility across every leg of the sequence from a single interface. If a DME delivery is delayed, the system flags it before the patient arrives home without equipment.
The Value-Based Care Connection
For health systems under ACO contracts, bundled payment programs, or Medicare Advantage risk arrangements, care transition performance is contract performance. Readmission rates, care transition completion, and average length of stay all feed directly into payer settlements and shared savings calculations.
VectorCare Insights provides readmission-rate analytics that correlate logistics failures with bounce-back risk — giving care teams a clear view of where coordination gaps are creating financial exposure.
What's Driving AI Adoption in Hospital Scheduling
Three forces are converging to make AI scheduling automation a near-term priority for most health systems:
Workforce and Cost Pressure
Hospital workforce costs rose 5.6% in 2025, with total labor spend exceeding $1 trillion. McKinsey has estimated up to $265 billion in annual U.S. healthcare administrative savings are achievable through administrative simplification. AI scheduling tools capture a direct share of that opportunity by handling repeatable coordination tasks without adding headcount.
Value-Based Care Financial Pressure
28.7% of U.S. healthcare payments now flow through downside-risk contracts. When readmissions, extended stays, and care coordination failures carry direct financial penalties, automating the logistics that prevent them becomes a CFO-level priority — not just an IT initiative.
Technology Maturity
With 96% EHR adoption among acute care hospitals and FHIR-based APIs now standard, the integration prerequisites that once blocked AI scheduling adoption have been met. Platforms like VectorCare can embed directly into existing EHR workflows via SMART on FHIR — no rip-and-replace required.
VectorCare's hospital partners report savings of $500,000+ annually at larger facilities, with deployment ROI typically clearing in under 12 months — once scheduling labor savings, bed-throughput recovery, and reduced readmission penalties are factored in.
Frequently Asked Questions
How do you automate patient scheduling?
Integrate an AI scheduling platform with your EHR for real-time availability and automated data extraction, then layer in self-service booking, automated reminders, and intelligent routing. Starting with high-volume, low-complexity appointment types typically delivers the fastest time to value.
What scheduling software is HIPAA compliant?
HIPAA-compliant scheduling platforms require Business Associate Agreements, encryption of PHI in transit and at rest, role-based access controls, and audit logging. Look for platforms that also hold SOC 2 Type II certification — VectorCare carries both designations, which most hospital procurement teams require for EHR-embedded applications.
Which AI appointment scheduler is best for hospitals?
Hospitals with complex transport and post-acute coordination needs should prioritize platforms with deep EHR integration, multi-service orchestration, and HIPAA/SOC 2 compliance. General-purpose scheduling tools built for simpler clinical environments rarely handle that complexity well. VectorCare is purpose-built for exactly these multi-service hospital workflows.
How does AI reduce no-shows in hospitals?
AI identifies patients at elevated no-show risk using historical behavior and appointment characteristics, then sends personalized multi-channel reminders at optimized intervals. It also makes rescheduling frictionless through self-service, converting potential no-shows into filled slots rather than lost appointments.
Can AI scheduling systems integrate with Epic or other EHRs?
Yes. Modern platforms use FHIR-based interoperability standards, including SMART on FHIR apps available directly in the Epic App Orchard, to connect bidirectionally with Epic and other major EHRs. VectorCare's SMART on FHIR integration enables real-time data exchange without any manual re-entry.
What is the ROI of AI scheduling automation for hospitals?
ROI comes from multiple directions:
- Recovered staff hours from eliminated manual coordination
- Reduced revenue loss from no-shows and last-minute cancellations
- Lower administrative overhead and faster discharge throughput
- Fewer readmission penalties through better post-acute follow-through
VectorCare hospital partners report $500,000+ in annual savings at larger facilities, with ROI typically achieved within 12 months of deployment.