Introduction
Clinical teams are drowning in administrative work. Even as patient volumes climb and staffing stays tight, coordination still runs on phone calls, faxes, and manual follow-up. The numbers confirm what frontline staff already know: administrative expenses account for 15%–25% of total U.S. healthcare expenditures, representing an estimated $600 billion to $1 trillion annually. That's not a rounding error — it's a structural problem.
Clinical workflow automation gets discussed as a solution constantly. What gets discussed far less is what it actually changes on the ground — fewer delays, less time lost to manual follow-up, and patients moving through care with less friction at every handoff. Most coverage leads with vendor promises. This article leads with operational outcomes.
This article breaks down the specific advantages of clinical workflow automation — what it actually changes, what goes wrong without it, and how healthcare organizations can extract lasting value from it.
Key Takeaways
- Clinical workflow automation replaces manual, repetitive tasks across scheduling, documentation, care coordination, and patient transport with rule-based and AI-driven processes.
- The strongest results appear in three areas: reduced administrative burden on staff, faster and more reliable care transitions, and measurable cost reduction.
- Manual workflows compound over time, producing higher error rates, longer stays, and rising labor costs.
- Integration with existing EHR systems is non-negotiable — siloed automation creates new coordination problems, not fewer.
- Outcomes must be tracked consistently, not assumed — automation without measurement drifts from its intended function.
What Is Clinical Workflow Automation?
Clinical workflow automation is the use of technology to take over repeatable, manual steps in clinical and operational processes — so care teams spend less time on administration and more time on patients.
It applies across two broad domains:
- Intra-facility processes: documentation, scheduling, billing, lab routing, prior authorization
- Cross-facility coordination: patient transfers, transport dispatching, discharge planning, post-acute placement, home health referrals
That scope makes it relevant to hospitals, health systems, payers, post-acute providers, and NEMT coordinators alike.
Automation as Infrastructure, Not a Feature
Automation isn't a tool that replaces one task. It's a system that connects the steps between tasks — routing the right information to the right person without requiring a staff member to trigger each handoff manually.
VectorCare's founding philosophy captures this distinction directly. CEO David Emanuel built the platform on the premise that patient logistics is an infrastructure problem, not a scheduling problem. A better dispatch calendar doesn't fix fragmentation between systems. Infrastructure that connects them does.
That distinction changes how automation should be evaluated. The right question isn't which features a platform offers — it's whether the system eliminates the coordination gaps that cause delays, errors, and unnecessary labor.
Key Advantages of Clinical Workflow Automation
The three advantages below are grounded in operational and financial outcomes. Each ties to metrics healthcare leaders actively track: staff time, patient throughput, cost, and care quality.
Advantage 1: Reduced Administrative Burden on Clinical Staff
The most immediate effect of automation is the elimination of repetitive manual tasks — phone-based coordination, redundant data entry, manual dispatching, status follow-up — that consume staff time without adding clinical value.
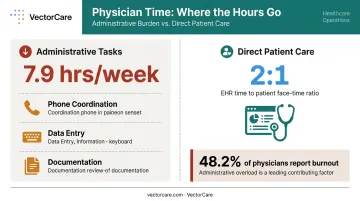
The scale of this burden is significant. According to AMA data, physicians in 2023 reported 7.9 hours per week on administrative tasks and 14.1 hours on indirect patient care — against a 59-hour workweek. Nearly half (48.2%) reported at least one burnout symptom.
Earlier research reinforces the pattern: physicians spend nearly 2 hours on EHR and desk work for every 1 hour of direct patient care.
How automation changes this: By replacing manual hand-offs with rule-based and AI-driven triggers, platforms can process requests, assign tasks, send communications, and update records automatically — without requiring a staff member to initiate each step.
VectorCare's A.D.I. (Automated Dispatching Intelligence) demonstrates this at scale. Clients have reported a 90% reduction in manual coordination tasks, and the platform has saved healthcare systems over 100,000 hours — a concrete measure of what well-implemented logistics automation delivers in high-volume environments.
Why this matters operationally:
- Staff freed from administrative volume can redirect attention to complex, high-judgment work that automation cannot replace
- Reduced manual load directly correlates with lower attrition risk — burnout decreases when the administrative pressure does
- In staffing-constrained environments, each staff member is carrying disproportionate load; automation absorbs that excess without requiring new hires
KPIs impacted: Staff hours on manual coordination, administrative error rate, time-to-task completion, employee retention and burnout scores.
When it matters most: Multi-department or multi-facility operations, high coordination volume, and organizations experiencing staffing shortages.
Advantage 2: Faster, More Reliable Care Coordination and Patient Transitions
Care coordination — especially at transition points like hospital discharge, interfacility transfer, and post-acute placement — is one of the most delay-prone phases in the care continuum. The handoffs are complex, communication gaps are predictable, and the downstream costs are measurable.
Nearly 20% of patients experience adverse events within 3 weeks of discharge, with almost three-quarters classified as preventable or ameliorable.
Discharge timing compounds the problem. Structured throughput initiatives have shown that discharges within 90 minutes of order improved from just 26.2% to 38.1% — most facilities start well below even that threshold.
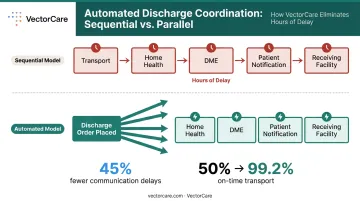
How automation changes this: Automated workflows trigger next steps the moment upstream criteria are met. When a discharge order is placed, the following can launch simultaneously rather than sequentially:
- Transport coordination
- Home health scheduling
- DME delivery
- Patient notification
- Receiving facility communication
That parallel execution eliminates the sequential delays that add hours to discharge timelines and keep beds occupied longer than necessary.
The operational case:
- Reducing coordination delays directly shortens length of stay — one of the highest-leverage metrics for hospital financial performance and bed capacity
- Better coordination prevents patients from falling through the cracks between care settings, reducing readmission risk
- Average readmission costs $16,300, which is 12.4% higher than the original index admission. Each prevented readmission is a concrete financial win
VectorCare's platform addresses this at the infrastructure level, connecting transport coordination, post-acute placement, and DME referrals into a single workflow rather than three parallel phone trees. Clients using the platform have reported a 45% decrease in communication-related delays and improvements in on-time transport performance from 50% to 99.2%.
KPIs impacted: Length of stay, time from discharge order to patient departure, on-time transport performance, readmission rate, care gap rate.
When it matters most: High-census hospitals, transfer centers managing complex referrals, health systems with large post-acute networks, and payers under value-based care contracts where readmissions affect reimbursement.
Advantage 3: Lower Operational Costs and Measurable Financial Impact
Automation reduces costs in two ways: it cuts the direct cost of labor-intensive manual processes, and it reduces the downstream costs of errors, delays, and rework that accumulate when workflows are fragmented.
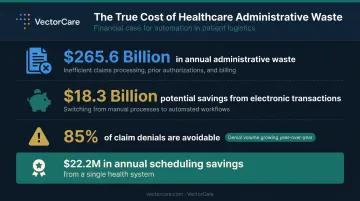
The financial stakes are not small. According to JAMA research, administrative complexity alone accounts for an estimated $265.6 billion in annual U.S. healthcare waste. The CAQH 2023 Index Report found the medical industry could save $18.3 billion simply by moving eligible administrative transactions to fully electronic processing.
Claim denials compound the problem further: 11% of all claims were denied in 2022, with 85% of those denials classified as avoidable — and the dollar value of denials increased 67% in that year alone.
How automation changes this:
- Processes tasks at scale with consistency that manual workflows cannot match
- Reduces denial rates by eliminating the documentation errors and timing failures that trigger them
- Shortens revenue cycles by accelerating prior authorization and billing workflows
- Prevents costly delays that extend length of stay and downstream care costs
Financial impact in practice:
- Cost savings compound over time — automation eliminates recurring errors rather than just addressing them after the fact
- For CFOs and health system leaders, automation ROI can be modeled, tracked, and presented in budget conversations
- VectorCare clients have reported an average of over $500,000 in annual savings per hospital partner, driven by scheduling efficiency, reduced coordination overhead, and improved transport cost management
One documented example: a health system processing over 900,000 service requests annually through VectorCare's platform achieved $22.2 million in annual scheduling time savings, growing transport volume by 40% without additional staffing costs.
KPIs impacted: Cost per discharge, administrative cost as a percentage of revenue, denial rate, time to payment, total cost of care.
When it matters most: Health systems under margin pressure, organizations with high payer mix complexity, and facilities facing labor cost increases without corresponding revenue growth.
What Happens When Clinical Workflow Automation Is Missing
Manual workflows create compounding problems that are difficult to reverse at scale.
When coordination depends on phone calls, faxes, and individual follow-up, errors accumulate silently. Delays become normalized. Staff develop workarounds that mask systemic problems without solving them.
The further an organization grows without automation, the harder those problems are to fix.
The consequences show up consistently across healthcare settings:
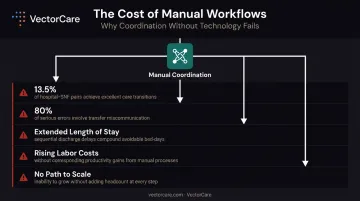
- Only 13.5% of hospital-SNF pairs report excellent performance across all dimensions of care transition information sharing — and 30% report poor performance
- An estimated 80% of serious medical errors involve miscommunication during patient transfers, per Joint Commission data
- Discharge delays persist when downstream coordination — transport, DME, home health — is managed sequentially by phone, extending length of stay
- Rising labor costs — more staff time absorbed by tasks automation could handle, without proportional productivity gains
- Inability to scale — manual coordination creates a ceiling on growth; adding volume requires adding headcount
Organizations that treat coordination as a staffing problem keep adding headcount without changing outcomes. The inefficiencies don't shrink — they just cost more.
How to Get the Most Value from Clinical Workflow Automation
Implementation strategy matters as much as platform selection. A few principles separate organizations that extract lasting value from those that deploy automation and see limited impact.
Start With High-Friction, High-Volume Workflows
Don't automate everything at once. Identify the workflows that produce the most delays, errors, or staff frustration — discharge coordination, transport dispatching, prior authorization — and start there. Early wins build organizational confidence and generate the outcome data needed to justify broader rollout.
Integration With Existing Systems Is Non-Negotiable
Automation tools that operate in silos create new coordination problems. Prioritize platforms that connect to your EHR through standardized protocols so patient data flows automatically without manual re-entry.
VectorCare's SMART on FHIR integration with Epic illustrates this directly: the platform reads demographics, clinical data, and discharge orders the moment they're entered, triggering logistics coordination automatically. Care coordinators stay in their existing workflow while the logistics infrastructure runs in the background.
Most FHIR integration layers of this type take 4–8 weeks to design, integrate, test, and validate — a manageable timeline relative to the ongoing coordination gains.
Track Outcomes Consistently — Don't Assume Them
Define the KPIs that matter before implementation. Then measure them at structured intervals:
- Baseline: Capture current performance before go-live
- 30 days: Confirm the system is functioning as configured
- 90 days: Evaluate real operational impact and identify drift
Automation that isn't monitored drifts. Workflows evolve, edge cases accumulate, and teams gradually revert to manual workarounds without anyone flagging it.
Organizations that sustain results treat automation as an ongoing operational practice — with designated ownership, regular review cycles, and a clear escalation path when performance slips.
Conclusion
The value of clinical workflow automation shows up in specific, trackable places: staff hours reclaimed from manual coordination, patients moving faster through care settings, lower administrative costs, and fewer errors at high-stakes handoff points.
The longer automation is applied consistently and reviewed regularly, the more an organization accumulates efficiency gains that would be impossible to achieve manually at scale. VectorCare's hospital partners, for example, average over $500,000 in annual savings — not from a single initiative, but from compounding improvements across dispatch, discharge coordination, and transport logistics. Organizations that start building that infrastructure today will have a measurable cost and quality advantage in 18 months. Those that wait will have a harder gap to close.
Automation isn't a one-time project — it's operational infrastructure. Like any infrastructure, it needs governance and ongoing iteration to stay aligned with how care delivery actually evolves. The organizations seeing the greatest returns treat it that way from day one.
Frequently Asked Questions
What is clinical workflow automation in healthcare?
Clinical workflow automation uses technology to standardize and take over repetitive clinical and operational tasks — scheduling, documentation, care coordination, patient handoffs — so staff can focus on higher-value care. It replaces manual, phone-based processes with rule-based and AI-driven triggers that move information and tasks automatically between people and systems.
What are the most common clinical workflows to automate?
The highest-impact starting points are patient intake and scheduling, clinical documentation, discharge and care transition coordination, patient transport dispatching, billing and prior authorization, and post-discharge follow-up communications.
How does clinical workflow automation reduce hospital costs?
Automation eliminates labor-intensive manual steps, reduces errors and the rework they require, shortens length of stay by accelerating care transitions, and decreases administrative overhead — including claim denials.
What happens if healthcare organizations delay adopting clinical workflow automation?
Manual workflows produce inconsistent outcomes and normalize delays. Staff burnout increases as administrative volume grows. Operational costs rise, and the gap between early adopters and laggards in care quality and financial performance widens.
How does clinical workflow automation affect patient outcomes?
Faster care transitions reduce exposure to hospital-acquired risks. Better coordination prevents patients from falling through the cracks between care settings. Reduced errors at handoff points — where the majority of serious medical errors occur — lower readmission rates and adverse events after discharge.
What should healthcare leaders look for when choosing a clinical workflow automation platform?
Prioritize EHR integration capability (FHIR-based, not proprietary), HIPAA compliance, the ability to coordinate across facilities and care settings — not just within a single department — scalability to handle high-volume environments, and documented outcomes from comparable organizations.