Introduction
For every hour a physician spends with a patient, research shows they spend nearly two additional hours on EHR-related tasks — documentation, data entry, and inbox management. That ratio, documented by Sinsky et al. in the Annals of Internal Medicine, reflects a system badly out of alignment with its own purpose.
The burden doesn't stop at clinician frustration. It cascades into delayed discharges, miscommunicated orders, extended lengths of stay, and burnout rates that now affect 45% of U.S. physicians. For hospital administrators and clinical leaders, these aren't abstract concerns: they're operational and financial realities showing up in throughput data every day.
This guide covers what EHR workflow optimization actually means in practice, the most common bottlenecks slowing care teams down, and specific strategies organizations can implement right now — including why care coordination workflows outside the EHR must also be addressed to fully capture efficiency gains.
Key Takeaways
- Physicians spend nearly 2 hours on EHR tasks for every 1 hour of patient care — optimization directly recovers that time
- Alert fatigue is measurable: medication alert override rates reach 93%, signaling broken clinical decision support
- FHIR-based integrations (SMART on FHIR) allow third-party tools to operate inside the EHR — eliminating system-switching
- Clinician involvement in workflow design isn't optional; IT-only redesigns consistently underperform
- EHR gains stall at discharge without automated logistics coordination to replace phone calls and manual handoffs
What Is EHR Workflow Optimization?
EHR workflow optimization is the ongoing process of configuring, customizing, and improving how EHR systems support clinical and administrative tasks — reducing friction, eliminating redundant steps, and aligning system behavior with how care teams actually work.
Optimization is distinct from implementation. Implementation gets the EHR live. Optimization makes it functional for the people using it daily.
Why "Set It and Forget It" Fails
Without continuous optimization, even well-designed EHRs underdeliver. Systems configured at go-live quickly fall out of sync with evolving clinical needs, specialty workflows, and user behavior patterns. The result is a familiar set of downstream problems:
- Poor usability that slows clinical staff down
- Workarounds that bypass the system entirely
- User fatigue and burnout from friction-heavy tasks
- Documentation errors that create downstream risk
Effective optimization is a cycle — driven by real-time feedback, audit log data, and iterative refinement. It requires governance structures, clinician input, and measurable targets.
Common EHR Workflow Bottlenecks Slowing Healthcare Teams Down
Documentation Burden
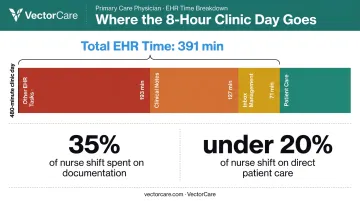
Primary care physicians now spend an average of 391 minutes per 8-hour clinic day in the EHR — over 6.5 hours. Of that, roughly 127 minutes goes to clinical notes and 71 minutes to inbox management. Medical-surgical nurses aren't spared either: studies show they spend 35% of their time on documentation and under 20% on direct patient care.
EHR interfaces were largely designed around billing and compliance requirements, not clinical efficiency. The result is high-volume, structured data entry that interrupts rather than supports care delivery.
Alert Fatigue
When every alert looks urgent, none of them do. Research from Bryant et al. found that clinicians override 93% of all medication alerts — with drug-drug interaction overrides reaching 95.1%. Even exact drug-allergy matches get dismissed 76% of the time.
This isn't clinician negligence. It's a rational response to systems that generate indiscriminate alerts based on population-level rules rather than patient-specific context. The consequence is dual: workflow interruption and genuine safety signals buried in noise.
Fragmentation Across Systems
Most healthcare organizations layer multiple external tools on top of their primary EHR. Each system switch adds cognitive load and creates opportunities for data loss. Common platforms a single care coordinator might navigate include:
- Pharmacy and medication management portals
- Scheduling and referral systems
- Discharge planning and transport coordination tools
- Billing and logistics software
For a single patient transition, teams may toggle between four to six of these platforms, filling gaps with phone calls, faxes, and manual status updates. Data silos form, re-entry errors accumulate, and no single system holds the complete picture.
Strategies to Optimize EHR Workflows
Streamline Documentation with Templates and AI-Assisted Tools
Structured clinical templates reduce documentation time by pre-populating predictable fields for common case types — particularly valuable in high-volume specialty settings. They work best for straightforward encounters; complex, multi-comorbidity cases still require substantial free-text input.
Ambient AI scribes represent a bigger shift. A 2025 study published in JAMA Network Open found that ambient AI documentation tools reduced physician documentation time by 27.7%. These NLP-powered tools capture physician-patient conversations in real time and convert them into structured notes within the EHR — dramatically reducing manual entry.
The limitations are real and worth stating plainly:
- Integration maturity varies significantly by EHR vendor and clinical setting
- AI-generated notes can contain fabricated content, requiring physician review
- Privacy, consent, and bias concerns require institutional governance before deployment
- Change management and training needs are non-trivial
Large language models are also being applied to patient inbox message drafting, helping clinicians respond faster to high-volume message queues. Responsible deployment here requires the same oversight — speed without governance creates a different kind of risk.
Reduce Alert Fatigue Through Smarter Clinical Decision Support
The shift from rule-based alerts to context-aware clinical decision support (CDS) is the most direct path to reducing alert fatigue. Well-designed CDS presents actionable guidance at the right point in the workflow — not as a disruptive interruption to it.
Alert governance is the other half of the equation:
- Conduct regular audits of alert firing rates and override rates
- Suppress low-value alerts that generate noise without improving care
- Calibrate alert thresholds to the specific role and specialty of the clinician receiving them
- Establish clear ownership for ongoing alert lifecycle management

The goal isn't fewer alerts universally — it's high-signal alerts that clinicians actually act on.
Improve Interoperability Through FHIR-Based Integration
FHIR (Fast Healthcare Interoperability Resources) is HL7's next-generation standards framework enabling on-demand, bidirectional data exchange between the EHR and third-party systems. Unlike older HL7 v2 push models that batch-transmitted data on fixed schedules, FHIR APIs enable near real-time data access.
Adoption has reached broad scale: about 9 in 10 U.S. hospitals enabled APIs for data sharing between EHRs and third-party technology in 2024, according to ONC.
SMART on FHIR takes this further. It allows external applications to launch within the EHR interface rather than requiring separate logins or browser tabs. For clinicians, this means a clinical decision support tool, logistics platform, or referral application can operate inside their existing workflow — not alongside it.
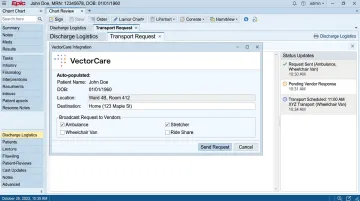
VectorCare's SMART on FHIR integration with Epic is a practical example. When a care coordinator initiates a transport or discharge logistics request, patient demographics, insurance information, encounter data, and clinical context are automatically pulled from Epic via FHIR APIs — no manual re-entry required.
The coordinator submits the request from within Epic, it reaches multiple transport providers simultaneously, and status updates flow back into the patient chart. The entire transaction is documented in the medical record without anyone typing a note.
That said, FHIR adoption alone doesn't guarantee workflow improvement. APIs must be standardized, well-governed, and embedded in ways that actually match clinical workflows — poorly integrated APIs add complexity rather than remove it.
Engage Clinicians in Continuous Workflow Design
EHR optimization fails when it's designed by IT teams in isolation. This isn't a criticism of IT — it's a structural problem. Clinicians are the ones absorbing the friction, and they're the only ones who can accurately identify where it originates.
Effective optimization requires structured, ongoing clinician input through:
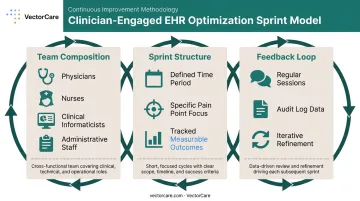
- Cross-functional sprint teams including physicians, nurses, clinical informaticists, and administrative staff
- Regular feedback sessions tied to specific workflow pain points
- Measurable sprint outcomes — not open-ended committees, but defined periods with tracked results
The University of Colorado's EHR optimization sprint program, documented by Sieja et al., demonstrated that targeted, clinician-engaged sprints over defined periods improved satisfaction and reduced EHR burden. The model works because it's specific, time-bound, and accountable.
Automate Repetitive Administrative Tasks
Administrative tasks consume a disproportionate share of clinician time. The AMA's 2025 prior authorization survey found that physicians and staff spend an average of 12 hours per week on prior authorizations alone.
Strong candidates for automation include:
- Appointment reminders and scheduling
- Prior authorization initiation
- E-prescribing and lab result routing
- Discharge follow-up scheduling
- Report generation
Smart defaults are an underutilized optimization lever. When EHR systems learn from user behavior and automatically correct recurring workflow inefficiencies — rather than forcing every user to manually override the same flawed default repeatedly — the cumulative time savings across a clinical team add up quickly.
Closing the Gap: From EHR Data to Care Coordination
Here's a problem that doesn't get enough attention: even a well-optimized EHR creates breakdowns the moment clinical decisions must translate into operational action.
Discharge planning is the clearest example. A physician documents a discharge order efficiently. The clinical note is clean, the data is structured. Then the care coordinator picks up the phone to arrange transport, calls a DME supplier, faxes a home health referral — and every efficiency gain made inside the EHR evaporates in the coordination process outside it.
This is where integrated patient logistics platforms that connect via SMART on FHIR extend EHR workflow efficiency into the post-clinical handoff. VectorCare's Epic integration addresses exactly this gap — rather than requiring coordinators to leave Epic to manage transport or discharge logistics in a separate system, the platform embeds that work directly in the chart:
- Patient data auto-populates from the existing record
- Vendors receive simultaneous broadcast requests in real time
- Status updates return to the EHR automatically, closing the loop
What previously took 31 minutes per logistics call — manual phone outreach, sequential vendor contact, data re-entry — compresses to under a minute with an embedded, automated workflow.
Those time savings have downstream consequences that matter to hospital leadership. Reducing length of stay and avoiding preventable readmissions depend as much on optimizing care coordination workflows as on clinical documentation efficiency itself. Discharge coordination failures don't register in EHR usability scores — they show up in throughput data and CMS penalty exposure.
How to Measure EHR Workflow Optimization Success
EHR-Focused Metrics
Track these at the individual and system level:
- Time-on-task for common documentation workflows (audit log data)
- Alert override rates by alert type, specialty, and clinician role
- Inbox message volume and time to resolution
- EHR session length per patient encounter
- After-hours documentation time ("pajama time") as a burnout proxy
Operational Outcome Metrics
Connect EHR efficiency to downstream patient flow results:
- Average length of stay and discharge delay rates
- Care transition completion times (order-to-departure)
- 30-day readmission rates
- Transport request-to-dispatch times
These metrics become most powerful when paired with EHR-level data. Alert governance that reduced override rates is useful on its own — but when that same governance correlates with shorter lengths of stay, the optimization program earns a budget line and executive attention.
Continuous Feedback Loop
Measurement doesn't stop once improvements are deployed. Each system update or clinical policy change can quietly erode gains — so ongoing feedback is what keeps the framework functional. Build in:
- Regular user surveys tied to specific workflows, not just general satisfaction
- Workflow audits aligned with system updates and clinical policy changes
- Periodic sprint reviews to assess whether prior improvements held or degraded
Frequently Asked Questions
What is the difference between EHR implementation and EHR optimization?
Implementation is the initial deployment of an EHR system — going live, training staff, and migrating data. Optimization is the ongoing process of refining how that system supports actual clinical workflows, addressing usability gaps, eliminating redundant steps, and adapting to user needs over time. Implementation is an event; optimization is a continuous discipline.
What are the most common causes of EHR workflow inefficiency?
The primary culprits are excessive documentation burden, alert fatigue from indiscriminate notifications, poor system usability, fragmentation across disconnected tools, and the absence of clinician input in system design and configuration. These often compound each other.
How does EHR optimization help reduce physician burnout?
By reducing time spent on manual data entry, simplifying documentation workflows, and eliminating low-value alerts, optimization lowers the administrative load that is a primary driver of clinician dissatisfaction. Research consistently links EHR usability and time burden to burnout rates.
What role does FHIR play in EHR workflow optimization?
FHIR enables standardized, on-demand data exchange between the EHR and integrated applications. SMART on FHIR takes this further by letting external tools operate within the EHR interface itself, eliminating separate logins and the system-switching that fragments clinical workflows.
How long does EHR workflow optimization take to show results?
Some improvements — alert tuning, template deployment, inbox routing changes — can show measurable results within weeks. Broader workflow redesigns and cultural shifts around clinician engagement typically take several months. Optimization is ongoing, not a one-time project.
How does patient transport and logistics coordination connect to EHR workflow efficiency?
Discharge and transport coordination are frequent breakdown points, where manual handoffs undo upstream efficiency gains. Integrating a logistics platform directly with the EHR via SMART on FHIR lets care teams initiate and track transport from within the same system, cutting coordination time and reducing delays at discharge.