Introduction
A missed scheduling coordination in healthcare can delay treatment, extend a patient's stay, or break an entire care pathway. In one analysis of preventable hospital delays, transport and scheduling failures accounted for a significant share of avoidable bed-days — problems no amount of clinical excellence can fix after the fact. That's what separates healthcare scheduling from scheduling in any other industry.
Automated patient scheduling solutions have become operational infrastructure across hospitals, health systems, payers, transport providers, and home health agencies. "Automated scheduling," though, describes tools that solve fundamentally different problems.
A self-service booking portal and a transport logistics dispatch platform are both "scheduling solutions." Choosing the wrong one for your actual bottleneck leaves the core problem unsolved.
This guide breaks down the three main types of automated patient scheduling solutions, what each one does, and how to identify which type maps to your organization's specific operational failures.
Key Takeaways
- Automated patient scheduling covers three distinct layers — self-service portals, clinical schedulers, and patient logistics platforms — and each one addresses a different operational problem.
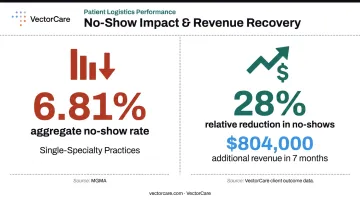
- MGMA data reports a 6.81% aggregate no-show rate for single-specialty practices — a measurable operational and revenue problem automation directly addresses.
- About 1.6 million patients are transferred between hospitals annually, making logistics coordination a high-volume, high-stakes function.
- Choosing the right solution starts with identifying your primary bottleneck, not evaluating technology sophistication or feature lists.
What Is Automated Patient Scheduling in Healthcare?
Automated patient scheduling is the use of software, AI, and system integrations to manage the coordination of patient appointments, transport, and care logistics — without requiring manual staff intervention for every routine task.
In practice, "scheduling" in healthcare spans three distinct layers:
- Patient-facing appointment booking — when and with whom a patient receives care
- Provider and resource matching — clinical routing, insurance verification, provider availability
- Operational care logistics — how and when patients physically move through the care system
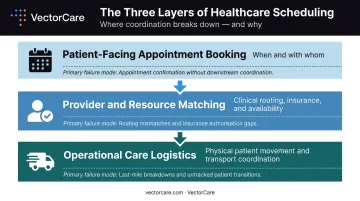
Each layer carries different failure modes and requires a different category of automation. Organizations that conflate them often invest in tools that solve the wrong problem entirely.
Across all three, the practical goal is the same: cut the coordination friction that consumes staff time, slows care delivery, and inflates operational costs.
Why Scheduling Automation Is Critical in Healthcare
Manual scheduling creates compounding failures at every layer. Phone tag between patients and schedulers, missed appointments from delayed reminders, care coordinators spending hours on transport calls — these aren't isolated inefficiencies. They compound across departments, facilities, and care transitions.
Consider what happens without automation at each level:
- Appointment layer: Slots go unfilled, no-shows erode revenue, front desk staff spend hours on inbound calls
- Clinical routing layer: Providers are mismatched, insurance issues surface at the visit, waitlists aren't managed
- Logistics layer: Discharge transport is delayed, beds stay occupied, home health visits are uncoordinated, clinical staff absorb administrative burden
The appointment layer alone carries measurable financial weight. MGMA reports an aggregate 6.81% no-show rate for single-specialty practices. At Memorial Hospital at Gulfport, closing that gap — a 28% relative reduction in clinic no-shows — generated $804,000 in additional revenue within seven months.
The logistics layer compounds those costs further. With average U.S. hospital expenses running $3,297 per adjusted inpatient day, every hour of discharge delay from uncoordinated transport carries a direct, measurable price tag.
Types of Automated Patient Scheduling Solutions
Automated patient scheduling is not a single product category. Solutions exist on a spectrum from basic self-service tools to complex logistics dispatch platforms. Large health systems often need solutions across multiple types simultaneously — particularly as care spans clinical, transport, and home-based settings.
Type 1: Online Self-Service Scheduling Portals
These are patient-facing digital portals or mobile apps that let individuals view available slots and book, reschedule, or cancel without calling the front desk. They run on calendar integration and fixed availability rules set by the practice.
These portals follow static rules with no clinical intelligence and no real-time coordination across systems. They present options; the patient or a rule engine makes the selection. There's no contextual reasoning or dynamic routing.
Best suited for primary care practices, preventive care programs, and small-to-mid-sized clinics where appointment types are simple and predictable. 48% of surveyed U.S. adults used online or mobile self-scheduling in the prior year, and more than 60% of patients prefer booking online over calling an office.
Key strengths:
- Reduces inbound call volume for routine bookings
- Provides 24/7 patient access without staff involvement
- Relatively low cost to implement
Limitations: Cannot handle clinical urgency, multi-provider coordination, or insurance complexity. Becomes a bottleneck when appointment types vary or when clinical rules require dynamic decision-making.
Type 2: AI-Powered Clinical Appointment Scheduling
These are conversational AI and machine learning systems integrated with EHRs. They interpret patient requests using natural language, match patients to the right provider and appointment type, verify insurance eligibility, apply clinical routing rules, and send proactive reminders without staff involvement for routine bookings.
Unlike portals, AI-powered clinical schedulers analyze context (patient history, provider specialty, insurance status, urgency signals) and dynamically route requests. Unlike logistics platforms, they focus on the clinical appointment layer, not post-appointment patient movement.
Best suited for multi-specialty health systems, high-volume clinics struggling with no-shows or phone tag, and organizations where provider-patient matching and clinical rule enforcement are the primary scheduling bottleneck.
Key strengths:
- Reduces no-shows through automated, personalized reminders via patient-preferred channels
- Fills cancelled slots via intelligent waitlist management
- Handles insurance verification and complex provider matching at scale
- Peer-reviewed research supports AI-based no-show prediction as an operational tool for reducing hospital cost impact
Limitations: Requires human oversight for clinical triage decisions and emergency routing. AI can enforce rules set by humans — it cannot exercise clinical judgment about appointment priority when symptoms are ambiguous. Complex multi-specialty sequencing still needs staff involvement.
Type 3: Automated Patient Logistics and Transport Scheduling
This is the most operationally complex layer of healthcare scheduling. These systems automate how patients physically move through the care system, covering non-emergency medical transport (NEMT), inter-facility transfers, air medical transport, discharge logistics, home health scheduling, and DME delivery coordination. The core function is multi-party, real-time dispatch — not calendar management.
Unlike Types 1 and 2, logistics scheduling must simultaneously coordinate patients, transport providers, receiving facilities, payers, and real-time vehicle or crew availability. It's a different kind of operational problem — which is why VectorCare's founder David Emanuel recognized patient logistics as an infrastructure problem rather than a scheduling problem when he was working in the ambulance industry.
The scale of this problem: MACPAC reports approximately 3.2 million Medicaid beneficiaries used NEMT in FY 2018, generating over 60 million ride-days. AHRQ estimates about 1.6 million patients are transferred between hospitals each year. These are high-volume, operationally complex movements that a clinical appointment portal cannot coordinate.
Best suited for hospitals managing high discharge volumes, transfer centers, NEMT providers, home health and DME agencies, payers coordinating member transport, and state or county health departments.
VectorCare's Automated Dispatching Intelligence (A.D.I.) is built specifically for this layer. The platform serves 2,500+ healthcare facilities, automates transport coordination from request through dispatch, integrates with Epic via SMART on FHIR, and has delivered a 90% reduction in manual coordination tasks for customers. In 2025, A.D.I. saved more than 100,000 hours across healthcare systems and suppliers.
The workflow shift is concrete: a transport scheduling task that previously consumed an average of 31 minutes of coordinator time (sequential provider calls, manual data entry, status follow-ups) is reduced to under three minutes through automated dispatch and real-time EHR integration.

Key strengths:
- End-to-end visibility across patient movement from discharge through transport to home or next care setting
- Real-time broadcast to provider networks — multiple qualified providers receive requests simultaneously rather than sequentially
- Reduces length of stay by eliminating transport coordination delays
- Supports multi-modal logistics: ground, air (including rotor-wing and fixed-wing), home health, and DME
- Over $500,000 in average annual savings per hospital partner, driven by labor cost reductions and faster bed turnover
Limitations: Requires deeper system integration across EHRs, transport provider networks, and payer systems. Implementation is more complex than clinical scheduling tools and demands organization-wide adoption to realize full coordination benefits. Organizations that treat this as a point solution rather than infrastructure will underutilize its capabilities.
How to Choose the Right Type of Automated Patient Scheduling Solution
The right type of automated scheduling solution is determined by your primary operational bottleneck. A hospital with a patient transport coordination crisis will not solve it with a clinical appointment scheduling portal, regardless of how AI-powered that portal is.
Diagnostic Questions to Guide Your Decision
Where are scheduling failures causing measurable harm?
- High no-show rates, front-desk call volume, appointment access complaints → Type 1 or Type 2
- Delayed discharges, transport coordination failures, extended length of stay, coordinator burnout from phone-based dispatch → Type 3
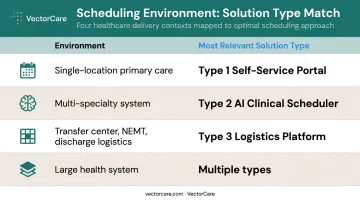
How complex is your scheduling environment?
| Environment | Most Relevant Type |
|---|---|
| Single-location primary care, simple appointment types | Type 1 |
| Multi-specialty system, provider matching, insurance routing | Type 2 |
| Transfer center, NEMT, discharge logistics, air/ground coordination | Type 3 |
| Large health system spanning all settings | Multiple types simultaneously |
What are your EHR integration requirements? Solutions that cannot write into your existing EHR in real time require staff to manually bridge gaps, which undermines any efficiency gain. For logistics platforms specifically, bidirectional FHIR integration — reading discharge orders and writing back transport status — keeps workflows connected rather than creating a parallel workaround that staff must maintain separately.
Who initiates the coordination?
- Patient initiates → Type 1 (self-service portal)
- Staff initiates for clinical routing → Type 2
- Multi-party coordination across transport providers, facilities, and payers → Type 3
Large systems typically need more than one type simultaneously, since clinical appointment automation and patient logistics automation address entirely separate operational gaps.
What to Check Before Finalizing a Scheduling Solution
Three common mistakes to avoid:
1. Overbuilding for the actual problem. Choosing the most technically advanced solution when a simpler type addresses the bottleneck adds implementation burden, cost, and staff resistance without proportional benefit. A small primary care practice doesn't need multi-party logistics dispatch.
2. Applying clinical scheduling tools to logistics problems. This is the most consequential error for hospitals and transfer centers. Clinical appointment scheduling and patient logistics scheduling are fundamentally different operational domains. Adapted appointment software cannot coordinate real-time multi-provider transport dispatch, regardless of how it's configured.
3. Skipping HIPAA compliance and integration verification. The HHS OCR 2023 annual breach report received 746 breach reports, with 63% originating from healthcare providers. Any scheduling solution handling protected health information must include:
- HIPAA-secure architecture and a signed Business Associate Agreement
- Encrypted data transmission and audit trail capabilities
Missing any of these creates regulatory exposure that no scheduling efficiency gain can offset.
Run compliance and integration checks during vendor evaluation, before contracts are signed.
Conclusion
Online self-service portals, AI-powered clinical appointment engines, and automated patient logistics platforms are not interchangeable. They each solve a distinct problem at a distinct layer of the healthcare coordination stack.
The organizations that realize the greatest gains correctly diagnose which layer is failing first — then match the right solution to that failure:
- Self-service portals fix the patient access layer: online booking, reminders, and intake forms
- Clinical scheduling engines fix the care sequencing layer: provider matching, slot optimization, and waitlist logic
- Patient logistics platforms fix the coordination layer: transport, discharge, NEMT, home health, and post-acute handoffs
Most delayed discharges, missed rides, and care gaps don't originate in the scheduling system. They originate in the logistics layer — and that's where platforms like VectorCare operate. Getting the diagnosis right determines whether an investment actually moves the needle.
Frequently Asked Questions
What is the most popular scheduling method in healthcare?
Phone-based scheduling still dominates — nearly 9 in 10 adults still use the telephone to schedule appointments at least some of the time. Online self-service portals are growing, with 48% of adults having used them in the prior year. For logistics-heavy organizations like hospitals and transfer centers, purpose-built transport automation is increasingly the standard, not an add-on.
What is automated patient scheduling in healthcare?
It's the use of software, AI, and system integrations to manage scheduling of appointments, transport, and care coordination tasks without staff manually handling each transaction. It covers everything from online booking portals to AI-powered clinical schedulers to automated patient logistics dispatch platforms, each targeting a distinct coordination layer.
How does automated scheduling reduce no-shows in healthcare?
Automated systems trigger personalized reminders via the patient's preferred channel, enable self-service rescheduling before a no-show occurs, and proactively contact waitlisted patients to fill cancelled slots — removing the friction that turns an inconvenienced patient into a missed appointment.
What is the difference between clinical appointment scheduling and patient logistics scheduling?
Clinical appointment scheduling coordinates when and with whom a patient receives care. Patient logistics scheduling coordinates how the patient physically gets there — covering transport, inter-facility transfers, NEMT, home health visits, and DME delivery. Each represents a distinct operational problem that requires its own purpose-built automation.
Is automated patient scheduling HIPAA-compliant?
Compliant solutions require a HIPAA-secure architecture, a signed Business Associate Agreement, encrypted handling of protected health information, and full audit trails. Verify these controls during vendor evaluation. Don't assume compliance after go-live.
What should healthcare organizations look for when choosing a scheduling automation solution?
Match the solution type to the specific operational problem first: appointment access versus patient movement are different problems. Then verify real-time EHR integration capability, confirm HIPAA compliance controls, and assess whether the vendor has experience in healthcare-specific workflows — not just general scheduling automation adapted for clinical settings.