This isn't an edge case — it's the daily operational reality at thousands of facilities across the US. And while "integration" gets discussed in every strategy meeting, it rarely gets defined in terms of what it actually changes for the people doing the work.
This article explains what integration in healthcare systems means in practice, the measurable advantages it produces across clinical and operational outcomes, and what compounds quietly when it's absent.
Key Takeaways
- Healthcare integration connects disparate systems so data flows automatically — eliminating manual re-entry, phone tag, and information gaps
- An estimated 60% of medication errors occur during care transitions — integration directly addresses this risk
- Medicare readmissions cost $26 billion annually, with $17 billion considered avoidable — poor care transitions are a primary driver
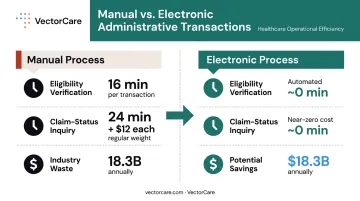
- Manual administrative transactions cost the healthcare industry billions each year — costs that full electronic adoption could largely eliminate
- Organizations that treat integration as core infrastructure — not a bolt-on — see measurable gains in efficiency, safety, and cost control
What Is Integration in Healthcare Systems?
Integration in healthcare means connecting the software, platforms, and workflows that different departments and providers rely on — so information flows instead of stalling.
In practice: a clinician shouldn't need five separate logins to get a complete picture of a patient. A receiving facility shouldn't be making admission decisions based on a faxed summary that's already 48 hours old.
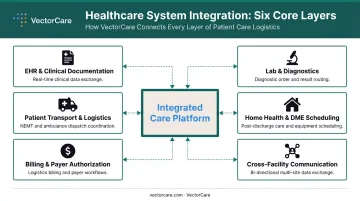
Integration applies across every layer of care delivery:
- EHR and clinical documentation systems
- Laboratory and diagnostic platforms
- Patient transport and logistics coordination
- Home health and DME scheduling
- Billing and payer authorization workflows
- Cross-facility communication and transfer centers
The measure of integration isn't whether systems are technically connected — it's whether care is faster, safer, and less expensive to coordinate as a result.
In 2023, only 43% of non-federal acute care hospitals routinely engaged in all four interoperability domains, and only 16% sent summary-of-care records to most or all long-term and post-acute care providers. That gap between having access to integration and actually using it is where most organizations lose value.
Key Advantages of Integration in Healthcare Systems
Advantage 1: Unified Data Access and Improved Clinical Accuracy
When systems are integrated, every authorized provider and coordinator sees the same patient — same history, same active orders, same transport status, same post-acute plan — from one interface. Data entered in the EHR reaches the transport team, the receiving facility, the home health scheduler, and billing automatically. No phone calls, no re-entry, no fax confirmations.
The clinical stakes are significant. A 2022 systematic review found that 18.1% of EHR safety events were linked to interoperability issues, with medication data involved in 20% of those incidents. The same review found that 64% of patients had discrepancies in hospital medication lists — including 43.9% with missing medications entirely.
This is what fragmented records produce in practice: clinicians and logistics teams making decisions from different, incomplete versions of the same patient.
KPIs this directly impacts:
- Medication error rates
- Duplicate test rates (one study found 32% of transferred patients received duplicate tests within 12 hours)
- Handoff quality scores
- Time-to-decision on transfers
- Clinical documentation accuracy
When this matters most: Multi-facility health systems, patients with multiple comorbidities, and any environment where care spans more than one provider or location. The more handoffs a patient experiences, the more opportunities fragmented data has to create harm.
VectorCare's SMART on FHIR integration with Epic addresses this directly — pulling patient data automatically into transport workflows so logistics coordinators and clinical teams work from the same real-time information, without toggling between systems.
Advantage 2: Operational Efficiency and Reduction in Manual Coordination Tasks
Every phone call to confirm a transport, every fax to transmit a record, every manual re-entry of scheduling data — these aren't minor inconveniences. They consume hours of staff time daily, introduce lag at every handoff, and compound as volume grows.
The numbers from CAQH put this in perspective: manual eligibility and benefit verification averages 16 minutes per transaction. Manual claim-status inquiries average 24 minutes and roughly $12 each. Full electronic adoption for nine administrative transaction types represents $18.3 billion in annual industry savings.
That's not administrative overhead. That's clinical capacity being consumed by coordination tasks that technology should be handling.
What integration changes in practice:
When a care coordinator initiates a patient transfer in an integrated system, the logistics platform automatically extracts relevant clinical data, identifies the appropriate transport level, and dispatches a provider — without a single phone call. VectorCare's SMART on FHIR integration with Epic demonstrates this model in deployment.
A regional hospital network in Ohio implemented VectorCare's Priority Dispatch protocols directly within Epic. ALS utilization dropped from 68% to 41% of inter-facility transports — a 27-percentage-point reduction that saved $2.1 million in year one. The driver was protocol-driven, system-embedded decision support replacing ad hoc dispatch calls made at the moment a transfer was initiated.
For a 250-bed hospital processing roughly 25 daily transports, VectorCare's platform reduces per-request scheduling time from approximately 31 minutes to under 3 minutes — a reduction that translates to over $500,000 annually in labor and bed costs.
KPIs this directly impacts:
- Time-to-transport initiation
- Staff hours spent on coordination
- Number of manual touchpoints per patient transfer
- On-time transport performance
- Length of stay (LOS)
When this matters most: High-volume transfer centers managing dozens of daily inter-facility moves, NEMT coordinators handling scheduled rides, and health systems coordinating post-acute placements across SNF, home health, and DME providers simultaneously. In those environments, manual coordination doesn't just slow throughput — it sets a hard ceiling on how many patients a team can move in a day.
Advantage 3: Continuity of Care and Reduced Readmissions
Care transitions are the highest-risk moments in a patient's episode of care. Not because clinical care gets worse at discharge — but because the information flow breaks down exactly when it matters most.
Only 12% to 34% of discharge summaries reach aftercare providers by the first follow-up appointment. That means most patients arrive at their next care setting before their clinical team there knows what happened.
The financial stakes are direct:
- 20% of patients experience adverse events after discharge — two-thirds considered preventable
- Medicare readmissions cost $26 billion annually, with $17 billion deemed avoidable
- ~20% of Medicare beneficiaries are readmitted within 30 days; a median 27% of those readmissions are preventable
- HRRP readmission penalties can reach a 3% payment reduction for facilities under CMS quality incentive programs

What integration changes here:
When transport, clinical notes, discharge instructions, scheduling, and payer authorizations are connected rather than siloed, care teams can identify transition gaps before the patient leaves — not after they bounce back. A Care Transitions Intervention study found a reduction in 30-day readmissions from 11.9% to 8.3%, saving $500 per case. A separate care transition team intervention reduced readmissions among contacted patients from 18% to 9%.
For facilities already operating under thin margins, those numbers hit twice: reduced readmissions improve outcomes and directly protect CMS reimbursement rates.
KPIs this directly impacts:
- 30-day readmission rates
- HCAHPS Care Transition composite scores
- Discharge-to-service time for home health and DME
- Average LOS
- Payer audit exposure
What Happens When Integration Is Missing
The costs of fragmentation compound in three directions simultaneously.
Operationally: Staff spend hours each day on manual coordination that integrated systems handle automatically. Phone calls to confirm transport. Faxes to transmit records. Duplicate data entry across platforms. None of these tasks add clinical value — and all of them scale with volume.
Clinically: Providers at receiving facilities make decisions based on incomplete information. One study found that 71% of hospitals had routine access to outside clinical information, but only 42% reported that clinicians actually used it during treatment. Access without use is the operational definition of a gap.
That gap creates conditions for medication errors, inappropriate care levels, and missed diagnoses — and makes meaningful quality review nearly impossible after something goes wrong.
Strategically: Organizations running on siloed systems struggle to scale, adapt to new care models, or respond to regulatory changes. They can't grow their transfer center volume without growing their coordination headcount. They can't add a new post-acute partner without creating new manual handoff points at the edges.
VectorCare was founded on a specific observation: patient logistics was being treated as a scheduling problem when it's actually an infrastructure problem. A scheduling solution optimizes the existing process. An infrastructure solution changes what the process can handle — more facilities, more volume, more care models, without a proportional increase in manual overhead.
How to Get the Most Value from Healthcare System Integration
Integration delivers its highest value when applied consistently across the full care continuum — not just within the hospital, but across transport, post-acute, home health, DME, and payer workflows. Partial integration doesn't solve the problem. It moves the handoff gap to wherever the connected systems end.
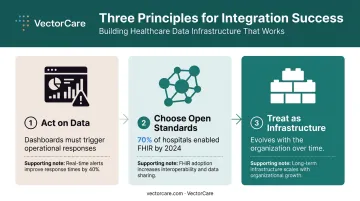
Three principles that determine whether integration delivers lasting value:
Act on what the data surfaces. Dashboards showing transport delays, readmission risk flags, or coordination bottlenecks only matter if they trigger operational responses. Reports that go unreviewed generate no ROI.
Choose open standards. By 2024, 70% of hospitals enabled access through HL7 FHIR-based apps. FHIR lets systems evolve as new vendors and workflows are added, without custom development at every turn. Proprietary, closed systems trade short-term convenience for long-term dependency.
Treat integration as infrastructure, not a project. A one-time implementation optimizes a moment in time. Infrastructure evolves with the organization, absorbs new partners, and becomes more valuable as more workflows connect to it.
VectorCare's 2026 launch of SoFaaS (SMART on FHIR as a Service) puts this principle into practice, enabling healthcare vendors to build, deploy, and scale EHR-embedded applications in weeks using shared open infrastructure.
The organizations that get the most from integration aren't necessarily the ones with the most sophisticated technology. They're the ones that commit to it as a permanent operational foundation and build their vendor decisions around that commitment.
Conclusion
The importance of integration in healthcare systems lies in the control, clarity, and consistency it brings to every layer of care delivery — from clinical decision-making to patient logistics to payer coordination. Its value shows up not in the technology itself but in the outcomes it enables: fewer errors at handoff, faster transfers, shorter stays, lower readmission rates, and staff spending their time on care rather than coordination.
Organizations that build connected infrastructure today reduce costs, improve quality scores, and scale care delivery as patient volumes and complexity grow. That advantage widens over time — disconnected systems don't just slow operations, they create compounding failure points that become harder to unwind.
The decision to integrate is, at its core, an operational one. It determines whether a healthcare system can reliably move patients, data, and resources in sync — or continue absorbing the cost of the gaps between them. Platforms like VectorCare are built on exactly that premise: that patient logistics isn't a scheduling problem, it's an infrastructure problem, and the infrastructure has to connect.
Frequently Asked Questions
What is integration in healthcare?
Healthcare integration refers to connecting disparate systems, platforms, and workflows — including EHRs, transport, billing, and care coordination tools — so that data and actions move consistently across departments and providers, reducing manual handoffs, eliminating redundant data entry, and enabling faster, more accurate decisions.
What are the 3 C's of integrative care?
The Commonwealth Fund identifies the 3 C's of seamless care as Consistency, Continuity, and Coordination — three principles that together describe a model where providers work from shared information, patients move smoothly across care settings, and care plans remain coherent regardless of who is delivering them or where.
What are the main types of system integration in healthcare?
The primary types include:
- Clinical data integration — connecting EHRs and patient records across care teams
- Operational and logistics integration — coordinating transport, DME, and home health scheduling
- Financial and payer integration — automating billing, prior authorization, and eligibility verification
- Interoperability standards — HL7 and FHIR protocols that let different systems share data without custom interfaces
How does EHR integration improve patient outcomes?
EHR integration gives all care team members — including logistics coordinators and transport teams — access to complete, real-time patient data. This reduces handoff errors, speeds up care decisions, and ensures that receiving facilities have what they need before a patient arrives rather than after.
What are the challenges of implementing healthcare system integration?
The most common barriers are legacy system incompatibility, lack of standardized data formats, staff adoption resistance, and vendor fragmentation. Platforms built on open standards like FHIR reduce these obstacles by allowing new systems and partners to connect without requiring custom-built interfaces each time.
How does integration in healthcare reduce costs?
Integration reduces costs by eliminating manual administrative tasks, reducing duplicate tests and unnecessary procedures, lowering readmission rates, and shortening average lengths of stay. For a mid-size hospital, the combination of scheduling automation and bed throughput improvement alone can translate to over $500,000 in annual savings.