Introduction
Patient care doesn't end when a physician signs a discharge order. Getting the right service to the right patient at the right time (whether that's a wheelchair van, a home health nurse, or a DME delivery) requires an entire coordination infrastructure operating behind the scenes. That infrastructure is what "direct-to-patient logistics" describes.
The American Hospital Association reported that average hospital length of stay increased approximately 19% in 2022 compared to 2019, contributing an estimated $6.8 billion in added hospital costs, much of it driven by delayed discharges, transportation bottlenecks, and fragmented post-acute placement.
When logistics fails, patients wait in acute beds they no longer need, costs climb, and incoming patients face reduced capacity.
This article breaks down what direct-to-patient logistics means in healthcare — the key concepts, the core challenges, and why solving this problem requires more than better scheduling.
Key Takeaways
- Direct-to-patient logistics spans transport, home health, NEMT, and DME — not just a single handoff
- Fragmented, phone-based coordination extends length of stay and consumes clinical staff time
- Matching the right transport resource to the right clinical need is complex and often done manually
- HIPAA compliance and prior authorization add regulatory layers to every logistics workflow
- EHR-integrated platforms and automated dispatching are reshaping coordination at scale
What Is Direct-to-Patient Logistics?
In healthcare, direct-to-patient (DTP) logistics refers to the coordinated system of services — transport, home health, NEMT, durable medical equipment delivery — that ensures patients receive the right care in the right setting, wherever they are in the care continuum.
This differs from how the pharmaceutical industry uses the same phrase. In clinical trials and drug distribution, "direct-to-patient" means shipping investigational products or medications to a patient's home. This article focuses on care coordination logistics: the operational layer that moves patients and arranges services on their behalf across hospitals, post-acute facilities, and home settings.
Why This Matters Now
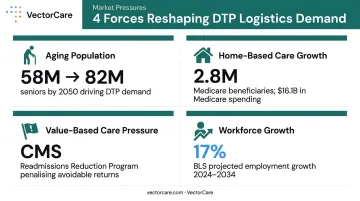
Several converging pressures are reshaping what DTP logistics demands from healthcare organizations:
- Aging population: KFF projects the U.S. population aged 65+ will grow from 58 million in 2022 to 82 million by 2050, driving significant increases in complex discharge and home care needs
- Home-based care growth: MedPAC reported approximately 2.8 million fee-for-service Medicare beneficiaries received home health in 2022, with $16.1 billion in Medicare spending
- Value-based care pressure: CMS's Hospital Readmissions Reduction Program penalizes hospitals with excess readmissions, making smooth care transitions a financial priority with direct reimbursement consequences
- Workforce signals: The BLS projects 17% employment growth for home health and personal care aides from 2024 to 2034 — reflecting demand that logistics infrastructure must keep pace with
The core goal of DTP logistics is coordinated handoffs across this entire continuum: from hospital discharge to NEMT pickup to home health visit, so no patient is lost in the gaps between providers.
Key Concepts Every Healthcare Operator Should Know
DTP logistics isn't a single handoff. It's a chain of coordinated events across acute care, sub-acute care, home health, ambulatory services, and transport providers — all of which need to communicate in real time. Several core concepts define how this chain is supposed to work.
Levels of Patient Transport
Not every patient needs the same vehicle. Transport level must match clinical need:
| Transport Level | What It Covers |
|---|---|
| ALS (Advanced Life Support) | Ground ambulance with ALS assessment or at least one ALS intervention |
| BLS (Basic Life Support) | Ground ambulance with medically necessary BLS services as defined by state |
| NEMT (Non-Emergency Medical Transport) | Scheduled transport for patients who need a medical vehicle but not emergency services |
| Rotor-wing (helicopter) | Air ambulance for time-critical transport where ground is insufficient |
| Fixed-wing (airplane) | Air ambulance for longer-distance critical transport |
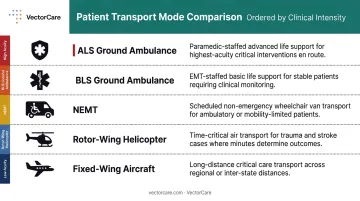
Mismatching transport level to clinical need creates two problems: sending an ALS crew for a routine discharge wastes a critical resource, while sending a wheelchair van for a patient who needs monitoring creates a safety risk.
Dispatch Coordination and Transfer Centers
Hospital transfer centers serve as the hub of transport coordination — receiving requests, evaluating patient acuity, identifying appropriate receiving facilities or transport providers, and managing communication between parties.
The volume is substantial. A survey of 32 U.S. tertiary care centers found a median of 700 transfers per month per institution, with some handling up to 2,500. Yet 84% of those institutions required a mandatory recorded three-way physician-to-physician call, and only 32% used their primary EHR to document transfers in real time. The infrastructure handling that volume is largely phone-based.
Prior Authorization and Payer Requirements
Before transport or home health services can begin, payers often require clinical documentation and explicit approval. For a process already measured in hours, that approval step adds friction. The AHA has documented that prior authorization in Medicare Advantage plans delays post-acute transitions and increases administrative burden on hospital staff — particularly for home health services.
Authorization failures don't just slow things down — they can result in denied claims or prolonged acute bed occupancy while facilities wait for approval. Those delays compound when real-time visibility is also missing.
Real-Time Visibility and Chain of Custody
Real-time visibility means knowing: Where is the patient? What transport resource is en route? What's the ETA? Has clinical handoff documentation been exchanged?
When visibility gaps exist — a coordinator doesn't know whether transport has been dispatched, or whether DME has been delivered to the home — the result is cascading delays:
- One party waits for confirmation that never comes
- Another makes a redundant phone call
- A discharge gets pushed by hours
The Core Challenges in Direct-to-Patient Logistics
The goal is straightforward: get the right service to the right patient at the right time. The execution is not. These are the categories of challenge that consistently create failures across the care chain.
Fragmented Communication Between Providers
A typical discharge event involves the sending facility, the receiving facility, the transport provider, the home health agency, and the payer, each using different systems and different communication channels. Phone, fax, and email don't interoperate.
The clinical staff burden is significant. McKinsey research found nurses spend 15% of a shift on charting and documentation, while a peer-reviewed time-allocation study put that figure closer to 25%.
Transfer center nurses in a qualitative study described performing "invisible work": filling information gaps, managing provider communication breakdowns, and keeping calls moving when clinical information wasn't shared upfront.
VectorCare's own operational benchmarks reflect this. Hospitals using manual coordination workflows saw nurses, social workers, and case managers spending over 45 minutes per patient making calls, completing paperwork, verifying insurance, and arranging transport. On the VectorCare platform, that process drops to under five minutes.
Regulatory and Compliance Complexity
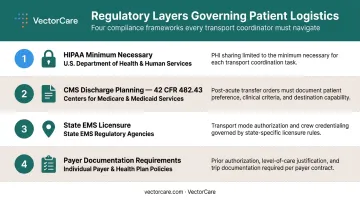
Patient logistics isn't just an operational challenge — it's a compliance one. Key regulatory layers include:
- HIPAA minimum necessary: HHS requires covered entities to use, disclose, and request only the minimum PHI needed for the intended purpose when sharing information with transport or home health providers
- CMS discharge planning: 42 CFR 482.43 requires hospitals to evaluate discharge needs and arrange post-acute transfers for patients at risk of adverse health consequences
- State EMS licensure: Transport providers operate under state-specific rules that vary considerably
- Payer documentation requirements: Each payer may require different clinical documentation before authorizing services
Non-compliance creates dual exposure: denied reimbursement and legal risk. Many facilities still route patient information through phone calls and faxes, channels that are inherently unsecured and poorly auditable.
Matching Transport Resources to Clinical Need
Resource matching sounds straightforward: find the right vehicle for the patient's condition. In practice, availability, geography, clinical capability, and cost all interact simultaneously. When done manually, coordinators call down provider lists hoping someone is available, then start over if they're not.
This process is slow. When it fails, patients stay in acute beds longer than necessary, occupying capacity the hospital needs for incoming patients. That same resource-matching gap falls on transfer center nurses, who coordinate transportation, bed assignments, and insurance approval simultaneously, often without real-time visibility into which providers are actually available.
Patient Privacy and Data Security
Every transport request requires sharing patient information with an external party. Every home health referral does too. The challenge is getting enough information to the right people, fast enough to be operationally useful, while meeting HIPAA's minimum necessary standard.
Many facilities still rely on fax and phone for this. Those channels are difficult to audit, prone to misdirection, and create significant compliance risk at scale. Secure, structured data exchange requires purpose-built technology, not workarounds layered on legacy infrastructure.
Scalability and Volume Surges
Patient logistics volume isn't constant. CDC data shows annual U.S. flu hospitalizations have ranged from approximately 100,000 to 710,000 in recent years, with significant seasonal concentration. Disaster events, facility closures, and mass-casualty incidents create sudden, unpredictable demand.
Manual, phone-based coordination cannot scale dynamically. When volume spikes, response times, accuracy, and throughput all suffer. Scheduling systems designed for steady-state conditions fail under surge precisely because they were never built as infrastructure.
Why Patient Logistics Is an Infrastructure Problem, Not a Scheduling Problem
VectorCare founder David Emanuel has argued for years that healthcare has fundamentally misclassified patient logistics. For decades, it's been treated as a scheduling task — handled case by case, one phone call at a time, by individual coordinators working in silos. The result is a system held together by institutional knowledge rather than integrated platforms.
What "Infrastructure" Actually Means Here
Just as a hospital depends on reliable electrical and IT systems, it needs reliable logistics infrastructure: a connected network of transport providers, home health agencies, DME suppliers, and communication systems that operates predictably at scale.
When logistics is treated as a back-office task, the burden falls on bedside staff. Nurses and case managers spend hours arranging transport rather than focusing on clinical care.
U.S. healthcare administrative spending runs an estimated $950 billion annually, with McKinsey identifying up to $265 billion in potential administrative simplification savings — logistics coordination is embedded throughout that figure.
Treating logistics as infrastructure produces different outcomes:
- 90% reduction in manual coordination tasks
- 45% decrease in communication-related delays
- Over $500,000 in average annual savings per hospital partner
- VectorCare's A.D.I. has saved healthcare systems and suppliers more than 100,000 hours by eliminating manual coordination

The Orange County Health Care Agency illustrates what this shift looks like. Before VectorCare, field staff spent up to 45 minutes manually calling down provider lists to confirm transport availability for mental health calls. After implementation, that coordination dropped to a fraction of the time — with more providers able to respond and fewer cancellations.
How Technology Is Reshaping Direct-to-Patient Logistics
The shift from phone-and-fax coordination to connected digital platforms is the central operational story in patient logistics right now.
EHR Integration and Interoperability
Modern logistics platforms integrate directly with EHR systems via SMART on FHIR, a standard that allows third-party applications to connect to EHR data and launch from within the clinical workflow. For Epic specifically, this matters at scale: KLAS-derived reporting puts Epic at 42.3% of U.S. acute care hospitals and 54.9% of beds as of 2024.
VectorCare's Epic integration pulls patient demographics, insurance information, and clinical context directly into the logistics workflow, eliminating redundant data entry and reducing errors. Clinical staff can initiate a transport request without leaving Epic, and the completed transaction writes back to the patient's medical record automatically.
Automated Dispatching
Manual dispatch means a coordinator identifies the need, calls a provider, waits for a response, and calls the next one if the first can't help. Automated dispatching broadcasts requests to an entire network of providers simultaneously, identifies the best available match based on availability and clinical need, and manages the response — all without a coordinator tied up on the phone.
VectorCare's Automated Dispatching Intelligence (A.D.I.) operates on this model. At Orange County Healthcare Agency, this approach doubled the number of ambulance providers able to respond to requests, reduced coordination time from 45 minutes to 4.5 minutes, and generated approximately $100,000 in annual savings on psychiatric transport calls alone.
Network Scale and the Value of a Connected Ecosystem
A logistics platform is only as effective as the network it connects. A dispatch tool with 10 providers in its network produces worse outcomes than one with 100 — because coverage, response time, and resource matching all improve with network depth.
Logistics should be treated as shared infrastructure, not a one-off integration. As more transport providers, home health agencies, and facilities join a common platform, the network effect compounds: faster response times, better resource matching, lower coordination overhead, and more reliable care delivery.
Frequently Asked Questions
What is a logistics nurse?
A logistics nurse — sometimes called a transfer or transport nurse — is a registered nurse who coordinates patient transfers and care transitions. They manage communication between referring and receiving facilities, arrange appropriate transport, and ensure clinical handoff documentation is complete before a patient moves.
What is direct-to-patient logistics in healthcare?
In healthcare, DTP logistics refers to the coordinated system of services — transport, NEMT, home health, and DME delivery — that ensures patients reach the right care setting after leaving a hospital or clinical facility. That destination could be a skilled nursing facility, a rehab center, or their own home.
What are the biggest challenges in direct-to-patient logistics?
Several operational gaps compound across the care chain:
- Fragmented communication between providers on different systems
- HIPAA compliance requirements when sharing patient data
- Manual coordination bottlenecks that slow discharge workflows
- Mismatches between transport resources and actual clinical need
- Phone-based processes that break down during volume surges
How does poor patient logistics affect hospital length of stay?
Delays in arranging transport, completing prior authorization, or securing post-acute placements keep patients in acute beds past their clinical discharge readiness. This reduces capacity for incoming patients and drives up cost — the AHA estimated delayed discharges added $6.8 billion in hospital costs in 2022 alone.
What technology is used to coordinate patient logistics?
Key tools include digital dispatch platforms, EHR-integrated logistics applications via SMART on FHIR, real-time tracking systems, and automated dispatching intelligence. Together, these cut manual coordination time, eliminate redundant data entry, and give care teams real-time visibility across the entire logistics chain.
What is NEMT and how does it fit into DTP logistics?
Non-Emergency Medical Transport provides scheduled, non-urgent transport for patients who need a medical vehicle but not emergency services — covering routine appointments, dialysis runs, and discharge transport. Approximately 3.2 million Medicaid beneficiaries used NEMT in 2018, and federal Medicaid rules require states to ensure this access for covered beneficiaries.