Scheduling sits at the center of this pressure. But the conversation rarely goes deep enough. Real-time patient scheduling gets described as a feature, a dashboard upgrade, or a nice-to-have. In practice, it's the difference between a patient leaving a hospital bed in hours or in days.
This article explains what real-time scheduling actually delivers — not in theory, but in the daily operational outcomes that matter to hospitals, transport coordinators, and care teams managing complex patient logistics.
Key Takeaways
- Real-time scheduling replaces phone-based coordination with automated, simultaneous outreach to all parties: transport, receiving facilities, and care teams
- The core operational wins are faster care coordination, shorter patient length of stay, and live visibility into where delays are happening
- Without it, care teams default to reactive firefighting: sequential calls, missed handoffs, and compounding delays
- Every hour of avoidable coordination delay occupies a bed — the average adjusted cost runs $3,025 per inpatient day in the US
- Organizations that treat real-time scheduling as infrastructure — not a feature — see the deepest operational returns
What Is Real-Time Patient Scheduling?
Real-time patient scheduling is a coordination system that surfaces live availability, automates requests, and confirms logistics across all parties simultaneously, eliminating the callbacks, faxes, and manual follow-up that slow care transitions down.
In plain operational terms: a discharge order goes in, and the system immediately broadcasts to available transport providers, notifies the receiving facility, and gives the care team a confirmed timeline. No phone tree. No sequential calls. No waiting to hear back.
Where It Applies
Real-time scheduling extends far beyond the clinical appointment slot. It applies anywhere a patient needs to move between care settings:
- Discharges — coordinating transport, home health setup, and DME delivery at the moment of clinical readiness
- Inter-facility transfers — connecting referring hospitals, transport providers, and receiving facilities in a single workflow
- NEMT coordination — managing non-emergency medical transport requests across a provider network
- Home health handoffs — triggering home health agency scheduling when a patient leaves the facility
- DME coordination — confirming equipment delivery before the patient arrives home
The CMS discharge planning regulation at 42 CFR 482.43 requires hospitals to arrange post-hospital care and avoid unnecessary delays. Real-time scheduling is how that requirement becomes operational — not just documented.
That distinction matters. Documentation of a discharge plan and execution of one are different problems. Real-time scheduling addresses the execution gap — the hours between a clinical decision and a patient actually moving.
Key Advantages of Real-Time Patient Scheduling
The advantages below are grounded in operational outcomes — most relevant to healthcare administrators, transport coordinators, and care teams handling high volumes of patient logistics daily.
Advantage 1: Faster, More Reliable Care Coordination
Traditional coordination is sequential. One team calls, waits, follows up, and escalates. The next step can't begin until the previous one confirms. This model doesn't just feel slow — the design makes it slow.
Real-time scheduling replaces that sequential chain with simultaneous, automated outreach. All relevant parties receive the request at once. Confirmations come back in real time. The care team gets a locked timeline without making a single call.
In practice, this matters more than it sounds. Research from AHRQ PSNet found that an estimated 80% of serious medical errors involve miscommunication during care transitions. The coordination gap isn't just an inconvenience — it's a documented patient safety risk.
To understand what this looks like at scale, consider VectorCare's 2024 platform activity:
- Processes a new logistics request every 23 seconds
- Sends network broadcasts every 12 seconds simultaneously
- Generated over 2.3 million broadcasts with a contract value exceeding $570 million
That throughput — sustained system-wide coordination, not just speed on a single request — is what separates a point solution from operational infrastructure.
KPIs impacted:
- Time from discharge order to patient departure
- Inter-facility transfer response time
- Staff hours spent on coordination calls
- On-time transport performance rate
When this matters most: High-volume transfer centers, hospitals with frequent inter-facility transfers, NEMT providers managing multiple simultaneous requests, and any system where coordination spans more than two parties.
Advantage 2: Improved Patient Access and Reduced Length of Stay
There's a gap between when a patient is clinically ready to leave and when they actually leave. In manual systems, that gap can stretch from hours to days. Real-time scheduling compresses it.
When transport, home health, DME, and receiving facilities are visible in a single real-time view, care teams confirm next steps at the moment of clinical readiness rather than after a round of calls. The coordination lag disappears, and so does the unnecessary bed day.
This carries real financial weight. The AHA reported that average hospital length of stay rose 19% in 2022 compared with 2019, driven in part by delays discharging patients to post-acute settings. Hospitals often received no reimbursement for those extra days after a patient was medically ready to leave.

With KFF data placing average adjusted hospital expenses at $3,025 per inpatient day, the cost of avoidable coordination delay adds up quickly across a health system's discharge volume.
Beyond cost, there's a patient experience dimension. A patient waiting hours for transport home, after being told they're medically cleared, notices. Timely coordination is a direct driver of satisfaction scores and HCAHPS outcomes.
VectorCare's SMART on FHIR integration with Epic addresses this directly: patient data flows automatically from the EHR into logistics coordination, reducing transport scheduling from 31 minutes to under one minute. The discharge order itself becomes the trigger for logistics, not a separate manual task.
KPIs impacted:
- Average length of stay
- Discharge-to-departure time
- Bed turnover rate
- Patient satisfaction (HCAHPS scores)
- Readmission rates
When this matters most: Hospitals managing bed capacity under pressure, SNFs with tight admission windows, PACE organizations managing complex patient transitions.
Advantage 3: Operational Visibility and Accountability
Real-time scheduling doesn't just move patients faster — it generates a live, auditable record of every coordination event, and that record is where accountability lives.
Without it, scheduling problems get diagnosed after the fact. After the delay. After the complaint. After the adverse event. Real-time visibility changes the model: administrators can see where handoffs are stalling and intervene before a delay compounds.
The safety stakes are well documented. Joint Commission Sentinel Event Alert 58 linked communication failures during care transitions to 1,744 deaths and $1.7 billion in malpractice costs over five years. Most were preventable, and most were invisible until something went wrong.
Real-time dashboards change that. VectorCare's platform surfaces active requests, pending confirmations, and performance data across the provider network, giving administrators a live picture of where the system is working and where it isn't. When every coordination event is timestamped and tracked, performance accountability becomes structural rather than retrospective.
The KPIs that shift when visibility improves:
- On-time performance rate
- Escalation frequency
- Coordination error rate
- Contract compliance by provider
- Average response time per broadcast
This matters most for large health systems managing multiple transport vendors, payers overseeing care coordination across a member population, and transfer centers handling time-sensitive patient movements.
What Happens When Real-Time Scheduling Is Missing
Many healthcare systems still run on phone, fax, and manual follow-up. Each party has an incomplete picture. The next step can only begin after the previous one confirms. At low volume, teams manage. At scale, this model breaks.
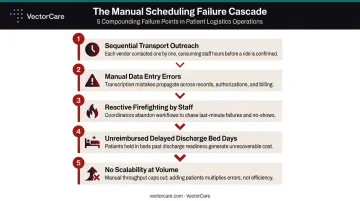
When it does, the consequences stack fast:
- Transport providers are contacted one at a time, creating avoidable waits while earlier vendors decline or don't answer
- Manual data entry across multiple calls introduces wrong-patient assignments, documentation gaps, and scheduling errors that increase liability
- Reactive firefighting — care teams spend hours per shift chasing confirmations rather than managing care, pulling nurses and case managers away from patients
- Delayed discharges and extended stays translate directly into unreimbursed bed days and staff burnout
- No scalability — a manual model that handles 10 daily transfers becomes unmanageable at 50; growth requires headcount, not efficiency
For many VectorCare customers, this looked like transport requests averaging 31 minutes per ride by phone or fax, faxed DME orders, mailed home health referrals, and no single source of truth on patient status. Orange County Health Care Agency reduced average transport arrangement time from 45 minutes to 4.5 minutes after implementing VectorCare — a 10x reduction.
How to Get the Most Value from Real-Time Patient Scheduling
Real-time scheduling delivers measurable returns when it's embedded across the care continuum , not used as a point solution for one department.
Three conditions determine how much value organizations actually capture:
EHR integration — Scheduling events should be triggered by clinical data, not by a staff member deciding to make a call. The infrastructure for this already exists in most health systems: in 2022, ONC reported that 69% of non-federal acute care hospitals used HL7 FHIR APIs for patient access, a 12-point jump from the prior year.
VectorCare's SMART on FHIR integration with Epic puts this to work directly: patient data is automatically extracted to initiate logistics coordination the moment a discharge order is placed, with no duplicate entry and no manual handoff between systems.
Consistent outcomes review — Real-time data is only valuable if teams act on what it reveals. On-time rates, bottleneck locations, and provider response times should appear in regular operational reviews , not only when something fails.
Shared platform visibility — When transport providers, receiving facilities, home health agencies, and DME suppliers all operate within the same platform, the "real-time" view is genuinely shared. When the hospital sees one picture and the transport provider sees another, coordination delays return regardless of the technology in place. Shared visibility is what makes the difference between tracking a problem and preventing it.
Conclusion
Real-time patient scheduling isn't an upgrade to an existing process. It replaces a coordination model that was never designed for the speed and complexity of modern care delivery.
The advantages compound. Faster coordination reduces length of stay. Shorter stays free capacity. Freed capacity reduces cost. Reduced cost enables better care. This cycle only sustains when scheduling is treated as ongoing operational infrastructure, not a one-time implementation.
The healthcare organizations that commit to this early gain a durable operational advantage — and the patients they serve experience fewer delays, fewer errors, and more timely access to the care they need.
Frequently Asked Questions
What are the main scheduling methods used in healthcare?
Healthcare uses several scheduling models — time-slotted, wave, open-access, urgency-based, and capacity-based. Real-time scheduling functions as an enabling layer across all of them, ensuring that availability, confirmations, and coordination updates happen instantly rather than through manual follow-up.
How does real-time patient scheduling differ from traditional scheduling?
Traditional scheduling is sequential and phone-dependent — one party confirms before the next is contacted. Real-time scheduling broadcasts simultaneously to all parties, confirms availability instantly, and updates all stakeholders automatically, cutting out the wait-and-follow-up loop.
What are the biggest barriers to implementing real-time scheduling?
The most common obstacles are legacy EHR systems that don't surface live data, fragmented vendor relationships that resist shared platforms, and staff habits built around phone-based coordination. Organizations that overcome these barriers typically start with EHR integration and a unified provider network.
How does real-time scheduling affect patient length of stay?
Real-time scheduling reduces LOS by compressing the gap between clinical readiness and actual care transition. When transport, home health, and receiving facilities are confirmed at the moment of discharge order, patients move within hours rather than days — eliminating the avoidable wait that drives unnecessary bed days.
Can real-time scheduling integrate with existing EHR systems?
Yes. Modern platforms support EHR integration through standards like SMART on FHIR, allowing scheduling events to be triggered directly by clinical data. VectorCare's Epic integration, for example, automatically pulls patient data to initiate logistics coordination without additional data entry.
What KPIs should healthcare organizations track?
Track these six metrics: discharge-to-departure time, on-time transport performance rate, coordination error rate, staff hours spent on scheduling calls, average provider response time, and patient length of stay.