Introduction
Home health care coordination sounds straightforward on paper: get the right clinicians to the right patients at the right time. In practice, it rarely works that way.
Nurses, therapists, aides, physicians, payers, DME suppliers, and family members often operate across completely separate communication channels — with no shared visibility into what anyone else is doing.
The consequences of that fragmentation are measurable. Research on Medicare home health patients found a 14.7% 30-day readmission rate — a benchmark that reflects, in part, what happens when care teams can't coordinate effectively after discharge. Missed visits, medication errors, delayed DME delivery, and regulatory citations follow the same pattern.
What follows is a practical look at what coordination actually requires — and what high-performing agencies do differently to close those gaps.
Key Takeaways
- CMS requires care coordination under 42 CFR 484.60 — poor documentation of coordination activities creates direct survey risk
- ~29% of hospitalizations with home health referrals don't result in care within 7 days of discharge
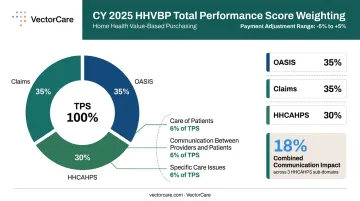
- HHVBP payment adjustments range from -5% to +5%, with communication domains carrying real financial weight in CY 2025
- Transport, DME delivery, and scheduling are clinical infrastructure — gaps in any one area directly delay patient recovery
- Automating logistics coordination has been shown to reduce manual coordination tasks by up to 90%, giving care teams time back for direct patient care
What Is Home Health Care Coordination?
Home health care coordination is the structured organization of care activities across everyone involved in a patient's home-based care: nurses, therapists, aides, physicians, family members, and payers. The goal is to ensure services are delivered safely, on time, and in the right sequence.
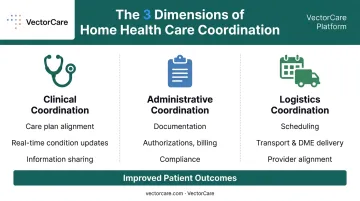
It spans three dimensions that most agencies still manage in silos:
- Clinical coordination: Ensuring clinicians share patient information, align on care plans, and communicate condition changes in real time
- Administrative coordination: Managing documentation, authorizations, billing, and compliance requirements across the care episode
- Logistics coordination: Scheduling visits, arranging transport, confirming DME delivery, and aligning multiple service providers around a single patient
Coordinated Care vs. Care Management vs. Case Management
These three terms are often used interchangeably, but they describe different scopes of work:
| Term | Focus | Scope |
|---|---|---|
| Care Coordination | Organizing activities across providers | Population-level; multiple providers |
| Care Management | Supporting individuals with acute needs | Individual; intensive clinical support |
| Case Management | Helping clients navigate systems | Individual; system navigation and advocacy |
Getting this right matters because these roles often overlap in practice. A patient transitioning from a SNF to home may simultaneously need case management to navigate insurance approvals, care management to stabilize a chronic condition, and care coordination to align the full clinical team across all three.
Every successful care episode depends on each of these participants staying in sync:
- Patient and family
- Home health clinicians
- Referring physicians
- Payers and insurers
- DME suppliers
- Transport providers
A breakdown at any point ripples across the rest — which is why coordination isn't just a workflow preference, it's a patient safety issue.
Why Effective Care Coordination Is Critical for Home Health Agencies
Patient Outcomes and Regulatory Compliance
When care teams share information in real time, chronic conditions are better managed, patients stay out of the hospital, and medication errors decrease. The 14.7% 30-day readmission rate among Medicare home health patients illustrates the stakes — and AHRQ research identifies communication failures during care transitions as a recurring patient safety risk, particularly in the critical post-discharge window.
Those outcome risks are precisely why CMS mandates care coordination as a Condition of Participation across three distinct regulatory standards:
- 42 CFR 484.60 — care planning and coordination of services
- 42 CFR 484.75 — skilled professional coordination
- 42 CFR 484.110 — clinical records
Surveyors look for both structured coordination (interdisciplinary team meetings, documented care planning) and unstructured coordination, such as clinician-to-clinician calls about condition changes. If those calls aren't documented in the medical record, they may as well not have happened from a compliance standpoint.
ACHC survey data confirms that care planning and coordination-related deficiencies under 42 CFR 484.60 are among the most frequently cited in home health surveys.
Financial Stakes Under HHVBP
Under the expanded Home Health Value-Based Purchasing model, CMS applies payment adjustments ranging from -5% to +5% to Medicare fee-for-service payments. In CY 2025, the Total Performance Score (TPS) is weighted 35% OASIS, 35% claims, and 30% HHCAHPS. Within HHCAHPS, the "Care of Patients," "Communication Between Providers and Patients," and "Specific Care Issues" domains each contribute 6% of TPS — 18% combined — making patient-reported communication quality a direct driver of payment.
Note: In CY 2026, HHCAHPS weighting drops to 20% and those three communication domains are removed from the measure set. Agencies tracking these metrics should distinguish between the two performance years.
Operational and Satisfaction Impact
Poor coordination creates non-billable time, scheduling gaps, and administrative overhead that erode agency margins. Families who feel the care team communicates well report higher satisfaction scores, while payers now tie coordination metrics to contract renewals and value-based arrangements.
Agencies that treat coordination as a core operational discipline — not an afterthought — are better positioned on every dimension that matters: outcomes, compliance, and revenue.
Common Challenges in Home Health Care Coordination
Siloed Communication and Documentation Gaps
Field clinicians often have no real-time access to updated care plans, medication changes, or notes from other team members. Without a unified information system, coordination decisions made at the point of care are invisible to the rest of the team and frequently go undocumented.
This creates a specific trap for clinical managers: coordination activities tracked in binders, sticky notes, or offline logs never make it into the patient record. When surveyors arrive, the coordination may have happened — but if it's not in the clinical record, the agency is exposed.
Care Transition Failures
The handoff from hospital or SNF to home is the highest-risk coordination point in the care continuum. The numbers reflect how often it goes wrong:
- Approximately 29% of hospitalizations with home health referrals did not result in home health care within 7 days of discharge31051-3/fulltext)
- Roughly one-third (33.5%) of home health episodes had delayed start-of-care nursing visits — despite CMS requiring the initial assessment within 48 hours of referral under 42 CFR 484.55
Delays in transport, late DME delivery, and incomplete referral packets can derail the first 48 hours of home-based care entirely. That window is when readmission risk is highest.
Logistics as a Hidden Bottleneck
Coordinating care for a single patient involves more moving parts than most agencies are built to handle:
- Scheduling skilled nursing and therapy visits around patient availability
- Confirming DME delivery windows before the patient arrives home
- Arranging non-emergency transport for follow-up appointments
- Aligning multiple vendors — each with their own systems and contacts
When all of this runs through phone calls, faxes, and disconnected spreadsheets, care teams burn hours on administrative follow-up. Clinical time shrinks, and coordination failures follow.
Effective Strategies for Home Health Care Coordination
Establish Structured Interdisciplinary Communication Routines
Regular, time-bound care coordination meetings are essential. Weekly or biweekly IDT meetings that include nurses, therapists, aides, and social workers create the structured forum where care plan changes, condition updates, and discharge planning actually get discussed.
A few specifics that matter:
- Include home health aides — they are the frontline eyes and ears of patient status changes, and excluding them from coordination meetings means missing critical clinical signals
- Offer virtual participation — field-based staff and agencies facing staffing shortages can't always attend in person; virtual options remove that barrier
- Time-box the meetings — open-ended coordination discussions become inefficient quickly; structured agendas keep teams focused
Standardize Documentation Across the Care Episode
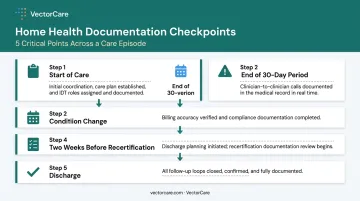
Define clear documentation checkpoints tied to key clinical moments:
- Start of care — initial coordination with the referring provider, care plan established, IDT roles assigned
- Any change in patient condition — clinician-to-clinician calls about status changes must be entered into the medical record, not just tracked verbally
- Final days of the 30-day billing period — documentation of coordination activities supports billing accuracy and compliance
- Two weeks before recertification — coordination and discharge planning conversations begin early enough to avoid last-minute gaps
- Discharge — all follow-up loops formally closed and documented
Clinical managers cannot carry the documentation burden alone. Delegate specific tasks to schedulers, operations staff, and support personnel so that coordination activities are captured consistently across every episode.
Prioritize Care Transition Coordination
Build a formalized protocol for every patient transitioning from hospital or SNF to home:
- Confirm transport is scheduled and on time before the discharge date
- Verify DME is delivered before the first clinical visit, not after
- Ensure the full referral packet — discharge summary, medication reconciliation, physician orders — is received and reviewed before the intake visit
- Formally close and document every follow-up loop
The first 48 hours are when coordination is most critical and most likely to fail. Without a defined protocol, that window becomes reactive by default — and reactive coordination is where readmissions start.
Integrate Logistics Coordination Into the Care Plan
Transition protocols only hold if the logistics behind them are tracked. Transport scheduling, DME delivery, and visit sequencing are not back-office tasks — they are clinical coordination. Each one can directly derail a patient's first days at home:
- A missing oxygen concentrator means the nursing visit can't proceed as planned
- An unconfirmed transport leaves a patient stranded at discharge
- An unreviewed referral packet means the intake visit starts without complete clinical information
When logistics are automated and tracked in real time, care teams can focus on patient care rather than chasing down confirmations. VectorCare's platform enables home health agencies and hospitals to automate patient transport requests and track logistics across the care continuum in real time, closing the documentation gaps that manual coordination creates.
How Technology Streamlines Home Health Care Coordination
EHR Integration and Real-Time Information Sharing
When coordination platforms connect to EHR systems via standards like SMART on FHIR, patient data flows automatically to every care team member — eliminating manual re-entry, version-control problems, and the "I didn't see that note" gaps that slow care down.
CMS's Post-Acute FHIR Orders project specifically includes electronic ordering of post-acute services — home health and DME — as part of its interoperability scope, signaling where the regulatory environment is heading. Agencies that build FHIR-compatible workflows now are better positioned for both operational efficiency and future compliance requirements.
VectorCare's SMART on FHIR integration with Epic enables bidirectional data exchange: patient demographics, acuity data, and clinical context flow into the logistics system automatically, while transport status updates and arrival confirmations write back to the patient chart (no phone calls required).
Automation Reducing Coordination Overhead
Once patient data flows reliably through integrated systems, the next bottleneck is the coordination work itself. Tasks like requesting transport, confirming DME, and tracking visit status are time-intensive — and highly automatable. Intelligent dispatching tools handle these logistics without manual intervention, freeing coordinators for the clinical judgment work that can't be delegated to software.
VectorCare's A.D.I. (Automated Dispatching Intelligence) has saved healthcare systems across hospitals, home health agencies, and transport providers more than 100,000 hours by automating patient logistics workflows — replacing the phone calls, manual follow-ups, and duplicate data entry that otherwise consume coordination capacity.
Key technology tools that address specific coordination gaps:
- Secure messaging and communication logs → replace fragmented phone calls, create auditable records
- Real-time alerts → flag condition changes immediately to the full care team
- Automated scheduling → reduce missed visits and scheduling conflicts
- Patient and family portals → keep families informed without adding to staff communication burden
- Audit-ready documentation → every logistics event is timestamped and structured, reducing survey exposure

Frequently Asked Questions
What is coordinated home health care?
Coordinated home health care is the deliberate organization of all care activities — clinical, administrative, and logistical — among every participant involved in a patient's home-based care. The goal is ensuring the right services reach the right providers at the right time, with no gaps from fragmented communication.
What does a home health care coordinator do?
A home health care coordinator manages communication among clinicians, physicians, payers, and families; oversees care transitions; monitors documentation compliance; and ensures all services — including transport and DME — align with the patient's care plan. In short, they're the single point of accountability keeping every moving part synchronized.
Does Medicare pay for care coordination?
Medicare covers Chronic Care Management (CCM) for patients with two or more chronic conditions lasting at least 12 months. Home health agencies must also satisfy CMS Conditions of Participation around care coordination to qualify for skilled home health reimbursement.
What is the 80/20 rule in home care?
In home care, a small percentage of high-acuity patients account for a disproportionate share of resource consumption and complications. Targeted coordination for that subset drives the most meaningful gains in both cost control and patient outcomes.
What are the biggest challenges in home health care coordination?
The most common obstacles are siloed communication, undocumented coordination that creates survey exposure, and care transition failures at discharge. Unmanaged logistics — delayed transport or late DME delivery — compound these problems during the critical first 48 hours at home.
How does technology improve home health care coordination?
Technology improves coordination through real-time EHR data sharing, automated scheduling, and auditable communication logs that give every care team member a unified view of patient status. Platforms like VectorCare connect transport, DME, and clinical scheduling in one place — eliminating the manual handoffs where gaps most commonly occur.