Introduction
Healthcare providers lose revenue, staff hours, and patient trust not from clinical failures but from scheduling breakdowns. A delayed discharge keeps a bed occupied. That occupied bed delays an ED admission. That ED backup elevates adverse event risk. The chain reaction starts with a missed transport window or a phone-tag loop that should have been resolved hours earlier.
The scale is real: outpatient no-show rates range from 12% to 42% depending on patient population and appointment lead time, and missed appointments cost the US health system an estimated $150 billion annually. Meanwhile, 94% of physicians report that prior authorization delays access to necessary care — adding another layer of unpredictability to already strained schedules.
Scheduling in healthcare is not an administrative nuisance. It is a systemic infrastructure problem. Left unaddressed, it degrades care quality, inflates costs, and burns out clinical staff. Fixing it means rethinking how patient movement is coordinated across every handoff — transport, discharge, home health, and beyond.
Key Takeaways
- No-show rates spike sharply when appointments are scheduled more than four weeks out — by 5.45x compared to same-day bookings
- ED crowding follows a predictable chain: discharge delays → bed unavailability → admission delays → patient safety risks from prolonged boarding
- Average hospital readmission costs $16,300 — 12.4% more than initial admissions
- Automated reminders, open-access scheduling, and transport coordination target different failure points — fixing one without the others leaves gaps
- Conflating patient logistics with appointment scheduling leads to coordination gaps that neither solution alone can close
Why Healthcare Scheduling Is a System-Level Problem
Most scheduling failures trace back to a supply-and-demand mismatch — but the real issue is how narrowly both sides of that equation are defined.
On the supply side, facilities typically count only the provider of record as "available." Open slots with other qualified clinicians, extended hours, or allied health providers go untracked.
On the demand side, the full patient need — including when they can actually get there, what transport they need, and what pre-authorization their payer requires — rarely factors into slot assignment.
The Provider-Centric Design Problem
Most scheduling systems are built around staff convenience and billing cycles — not patient need. The downstream effects compound quickly:
- Appointment types are standardized to fit administrative templates, not clinical reality
- Low-acuity patients crowd high-acuity slots because intake doesn't differentiate well
- Complex patients get squeezed into standard visit windows, creating overtime
- Care continuity suffers when visit length can't flex with clinical demand
The result: patients wait longer than necessary while capacity sits technically available but practically inaccessible.
How Failures Chain Together
The IOM framework for emergency department crowding categorizes delays as input, throughput, and output problems. Output delays — the inability to move admitted patients into inpatient beds — are often rooted in discharge coordination failures that have nothing to do with the ED itself.
A delayed discharge creates a bed shortage that backs up ED admissions and worsens crowding, which increases adverse event risk. Research across seven studies confirms that ED boarding is associated with reduced care quality and increased unfavorable patient outcomes.
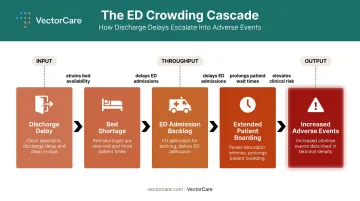
That chain makes clear why fixing scheduling at the department level rarely holds — the root cause is often two steps upstream.
The Benchmark Gap
Without visibility into where failures originate, measurement itself becomes a problem. There are no standardized national benchmarks for outpatient wait times or scheduling performance. Most facilities operate against internally defined targets — pragmatic thresholds set by historical norms, not evidence.
AHRQ has found insufficient empirical data linking even widely used metrics like Third-Next-Available Appointment to specific health outcomes. In practice, that leaves most facilities tracking activity rather than outcomes.
The Most Common Healthcare Scheduling Challenges
Physician Availability and Staff Constraints
In academic medical centers especially, providers carry competing clinical, educational, and administrative responsibilities. A department chief who's in committee meetings two mornings a week and supervising residents on a third effectively has a compressed scheduling window — and those gaps ripple into delayed patient access across the department.
No-Shows, Cancellations, and the Overbooking Trap
No-show rates are not uniform. A study of 263,464 appointments found an 8% overall no-show rate, rising to 13.6% for Medicaid patients. Appointments scheduled more than four weeks out carried 5.45x higher no-show odds than same-day bookings.
The administrative response — overbooking — creates its own problem. When most patients do show, providers face overtime, rushed visits, and deteriorating care quality. Neither underbooking nor naive overbooking solves the access problem; they trade one set of costs for another.
Fragmented Transport and Discharge Coordination
Scheduling failures don't stop at the appointment book — they extend into every handoff that follows. When a hospital arranges a patient transfer or discharge transport, the process often involves:
- Manual phone calls to multiple transport vendors
- Fax-based order transmission
- Separate systems for transport scheduling, EHR documentation, and insurance verification
- No real-time status visibility for the care team
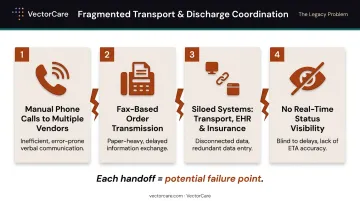
Each handoff is a potential failure point. A single missed confirmation can push a discharge to the following day — occupying a bed that another patient needs.
Multi-Specialist Coordination for Complex Patients
Patients managing multiple chronic conditions may need appointments with three or four specialists, across different facilities, with different scheduling systems. AHRQ has documented that fragmented care and insufficient coordination across providers create compounding communication gaps — and the burden of navigating that fragmentation typically falls on the patient or a single care coordinator with too many simultaneous cases.
Insurance Pre-Authorization Delays
Pre-authorization requirements inject unpredictable wait periods into scheduling workflows. For specialty care and non-emergency medical transport, this means a patient may be medically ready to proceed but administratively blocked. MACPAC notes that Medicaid prior authorization can limit access through both delays and outright denials — compressing the already narrow scheduling windows for Medicaid patients who also face higher no-show risk.
How Scheduling Failures Cascade Across the Care Continuum
The financial consequences of scheduling breakdowns are substantial and often underestimated.
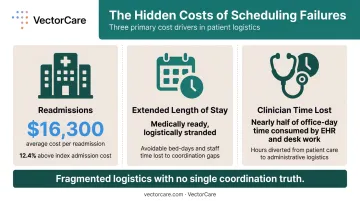
Readmissions are the most documented cost driver. AHRQ's Hospital Cost and Utilization Project reported that the average 2020 hospital readmission cost $16,300 — 12.4% higher than the $14,500 average index admission. When post-acute transitions (SNF placement, home health setup, DME delivery) aren't coordinated before discharge, readmission risk climbs.
Readmissions, though, are only part of the picture. Length of stay also extends when patients are medically ready but logistically stranded — transport unconfirmed, a DME order still pending, a SNF bed not yet secured. Each gap represents an avoidable cost: bed-days, staff time, and the next patient waiting for that room.
Clinician burnout compounds both. The time care coordinators spend on manual scheduling tasks — repeated phone calls, fax confirmations, status chasing — is a documented contributor to dissatisfaction in primary care settings. Physicians reported spending nearly half of their office-day time on EHR and desk work rather than direct patient care, time that better coordination workflows could return to the bedside.
These three cost drivers — readmissions, extended LOS, and clinician time lost to manual tasks — share a common root: fragmented logistics with no single source of coordination truth.
Proven Strategies to Improve Healthcare Scheduling
Standardize Workflows and Set Clear Scheduling Policies
Standard operating procedures for scheduling create consistency across staff and reduce preventable errors. Without SOPs, individual coordinators make ad hoc decisions that produce inconsistent patient experiences. With SOPs in place, staff spend less time improvising and more time handling the exceptions that genuinely need human judgment.
Effective scheduling SOPs should cover:
- Cancellation handling and same-day rebooking protocols
- Overbooking thresholds by appointment type and provider
- Buffer time allocation rules
- Escalation paths for scheduling conflicts
Adopt Data-Driven Capacity Planning
Historical demand data reveals predictable patterns: certain appointment types spike on Mondays, seasonal fluctuations affect specific specialties, certain patient populations book further in advance. Facilities that use this data to proactively staff and open slots avoid the reactive scramble when schedules break down.
Key metrics to track:
- Third-Next-Available Appointment (TNAA) by provider and specialty
- Overflow frequency — days when clinicians must work beyond standard hours to meet demand
- No-show rate by appointment lead time and payer type
- Cycle time from request to confirmed appointment
Implement Buffer Time and Contingency Protocols
Buffer slots — designated gaps between appointments to absorb late arrivals or extended visits — are not wasted capacity. They are the margin that keeps a schedule from collapsing when the first appointment runs long. Facilities that eliminate buffers in pursuit of maximum utilization often find they generate more overtime and worse patient experience than the utilization gain is worth.
Pair buffer time with active waitlist management: when a cancellation occurs, a structured waitlist process can fill that slot within minutes rather than losing the capacity entirely.
These outpatient strategies address the scheduling side of the equation. On the inpatient side, discharge and transfer coordination introduce a different set of delays — ones that no reminder system can fix.
Redesign Discharge and Transfer Coordination Processes
Discharge planning that begins the morning of discharge is already too late. Facilities that start the process at admission — identifying transport needs, SNF preferences, DME requirements, and home health eligibility — consistently move patients faster. Starting early means discharge orders don't stall while logistics catch up.
This requires coordinated workflows between:
- Clinical teams (who determine medical readiness)
- Bed management (who track capacity)
- Transport coordinators (who confirm logistics)
- Post-acute partners (who confirm receiving capacity)
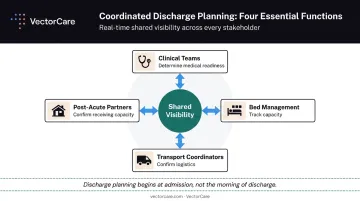
When these functions operate in separate systems without shared visibility, bed turnover slows, length of stay extends, and downstream capacity backs up.
Use Automated Reminders and Multi-Channel Patient Communication
Automated reminders work. A Cochrane systematic review found text reminders improved attendance versus no reminders (RR 1.10), and 62.5% of studies on open-access scheduling models reported significant no-show reductions. Shorter lead times and lower-friction rescheduling options reduce the cost of keeping an appointment.
Give patients channel choice — text, portal message, or phone — rather than a single call-in option. The friction of rescheduling by phone during business hours is a no-show waiting to happen.
How Technology and Automation Are Transforming Healthcare Scheduling
Modern scheduling platforms integrated with EHR systems through standards like SMART on FHIR eliminate manual data re-entry at the point of coordination. When a care coordinator initiates a transport request, the system automatically pulls demographics, pickup location, destination, and clinical context — compressing a process that previously took 31 minutes through phone and fax to under one minute.
This matters because coordinator time is finite. Every minute spent re-entering data that already exists in the EHR is a minute not spent managing exceptions, supporting patients, or confirming the complex transfers that actually require human judgment.
Automation Beyond Appointment Booking
The more significant shift is automation moving into logistics dispatching. AI-driven tools can now broadcast transport requests to available providers, handle timing and pricing negotiation, and confirm assignments without manual coordinator intervention.
VectorCare's Automated Dispatching Intelligence (A.D.I.) operates on this principle — automating the broadcast and confirmation cycle that previously required repeated phone calls. Across hospital partners, the platform has demonstrated a 90% reduction in manual coordination tasks and a 45% decrease in communication-related delays, with A.D.I. saving customers more than 100,000 hours in 2025 alone.

Coordinators who previously spent most of their day on the phone confirming transport can now focus on exceptions — the complex transfers that actually need human judgment.
Real-Time Visibility for Scheduling Leaders
Dashboards that surface live transport status, bed availability, and predicted demand change how scheduling leaders operate. Instead of reacting after problems have already cascaded — a patient still in their room two hours post-discharge order — leaders can spot the bottleneck forming and intervene before it delays the next admission.
Real-time visibility enables three practical actions:
- Early intervention: Flag delayed discharges before they affect bed availability
- Demand forecasting: Anticipate transport volume spikes by shift or day
- Accountability: Track on-time performance across transport vendors in one view
Johns Hopkins documented this approach with a command center model designed to manage patient flow from admission through discharge. The same logic applies whether you're running a 50-bed community hospital or a 500-bed health system: visibility precedes action, and early action costs far less than cleaning up a cascade that's already started.
Building a Culture of Continuous Scheduling Improvement
Process redesign and new technology only hold if leadership keeps them alive. Without structured feedback loops and active management attention, gains erode — often faster than they were built.
Organizations that achieve durable results do three things consistently:
- Review scheduling KPIs on a regular cadence — TNAA, no-show rates by payer and lead time, discharge delay attribution, and coordinator cycle time. Metrics that aren't reviewed don't drive behavior change.
- Pilot new scheduling models before system-wide rollout — Gains made without ongoing maintenance don't hold. One Massachusetts clinic network cut TNAA from 21 to 8 days within four months, then watched it climb back in four of five locations once active oversight lapsed.
- Include frontline staff in workflow redesign — Coordinators and schedulers know where the manual workarounds live. Process changes designed without their input tend to create new workarounds rather than eliminate old ones.
That maintenance requirement is the common thread across high-performing systems. The VA Amarillo system reduced next-available appointment time from 42.9 days to 15.7 days after implementing Advanced Access scheduling — a result that required both process redesign and sustained management commitment to hold.
Frequently Asked Questions
What are three factors that can affect appointment scheduling?
Physician availability and competing provider responsibilities, appointment type and duration variability, and patient-side factors including insurance status, transportation access, and no-show history. Prior no-show behavior alone increases future no-show odds by 4.42x, making it a reliable predictor worth tracking in any scheduling system.
What is the most common cause of scheduling delays in healthcare?
A supply-and-demand mismatch — facilities either underestimate true patient demand or define available supply too narrowly (counting only the provider of record, for example). This leaves capacity untapped while wait lists grow and patients face extended lead times that further increase no-show risk.
How does poor scheduling affect patient outcomes?
Scheduling failures contribute to delayed diagnoses, higher no-show rates, extended hospital stays, and increased readmission risk. Post-acute transitions involving transport, home health, or DME that aren't coordinated before discharge compound these effects — and ED boarding tied to discharge delays is directly associated with increased adverse events.
What is the difference between healthcare scheduling and patient logistics?
Appointment scheduling manages when patients are seen. Patient logistics encompasses how patients move through the care continuum — including transport, transfers, discharge placement, and NEMT coordination. Logistics is a broader infrastructure challenge that scheduling tools alone cannot solve, which is exactly the gap VectorCare built its platform to address.
How can hospitals reduce no-show rates?
The highest-impact interventions are automated multi-channel reminders, same-day or open-access scheduling models, and removing upstream barriers like transportation access and appointment lead time. Longer wait times directly correlate with higher no-show rates — cutting lead time from four-plus weeks to under one week can reduce no-show probability significantly.
What technologies help the most with healthcare scheduling challenges?
EHR-integrated scheduling platforms (particularly SMART on FHIR-certified tools), automated dispatching systems for patient transport, real-time bed and flow management dashboards, and AI tools that predict demand patterns and flag scheduling gaps before they become bottlenecks. The combination of appointment-level scheduling and logistics-level coordination is where the greatest efficiency gains emerge.