Introduction
When a patient is medically cleared for discharge but transport isn't arranged, a bed sits occupied. When a specialist is double-booked, a procedure gets delayed. These are daily occurrences across US healthcare systems — and the operational and financial costs add up quickly.
According to the American Hospital Association, average hospital length of stay was approximately 19% higher in 2022 than in 2019 — and nearly 24% higher for patients needing post-acute placement. Hospitals absorb those extra days without reimbursement.
Most organizations respond by refining their scheduling processes. But the real problem runs deeper. Fragmented tools, siloed data, and phone-based coordination point to an infrastructure gap — not just a process one. Patching workflows without addressing that gap means the same conflicts recur.
This article covers practical, proven strategies to prevent scheduling conflicts before they reach patients, resolve them efficiently when they do occur, and build the operational infrastructure that makes improvement stick.
Key Takeaways
- Scheduling conflicts are infrastructure failures — siloed systems and manual workflows — not individual errors.
- Centralized visibility, automation, and standardized escalation protocols are the most effective prevention tools.
- When conflicts occur, triage by patient care urgency first — logistics second.
- Tracking KPIs like on-time transport rates and time-to-resolution turns reactive firefighting into continuous improvement.
- Automating coordination and connecting systems through EHR integration closes the manual gaps where most conflicts start.
What Are Healthcare Scheduling Conflicts and Why Do They Matter?
A healthcare scheduling conflict is any situation where competing demands for staff, equipment, beds, or patient transport can't be fulfilled as planned. A double-booked specialist is the obvious example.
Less visible — and often more consequential — are patient logistics conflicts: a delayed transfer with no available transport, a discharge stalled because DME hasn't arrived, or a missed referral window when home health coordination falls through.
Two Types, One Root Problem
Most organizations track staff scheduling conflicts — overlapping shifts, coverage gaps, unplanned absences. These are visible and measurable.
Patient logistics conflicts are harder to see. Transport delays, bed unavailability, and uncoordinated discharge planning rarely show up in the same dashboards, yet they carry serious patient safety consequences. Research on critically ill interfacility transfers found that 28.37% of patients experienced clinical deterioration during transfer, rising to 63.27% among unstable patients. A missed transport window isn't an administrative failure — it's a clinical one.
The Downstream Consequences
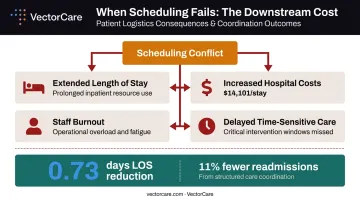
Scheduling failures don't stay contained. They cascade:
- Extended patient length of stay, consuming beds needed for incoming admissions
- Increased hospital costs — the average community hospital stay costs roughly $14,101, and every unnecessary day adds to that total
- Staff burnout from constant reactive coordination
- In serious cases, delayed time-sensitive care
A 2022 Cochrane review found that individualized discharge planning reduced length of stay by 0.73 days on average and cut unscheduled readmissions by 11%. Structured coordination produces real, quantifiable outcomes — and those outcomes compound across every patient, every shift, every facility.
Root Causes of Healthcare Scheduling Conflicts
Scheduling conflicts in healthcare rarely trace back to individual mistakes. The conditions that produce them are structural — built into how systems communicate, how staff are deployed, and how organizations hand off responsibility.
Siloed Systems and Fragmented Data
ONC data from 2024 shows 87% of hospitals integrated data for administrative tasks like scheduling and prior authorization — but only 35% used standards-based APIs to do it. That gap means the majority of hospital scheduling infrastructure still relies on non-standardized connections or, worse, no connections at all.
When scheduling data lives across phone logs, fax machines, spreadsheets, and separate EHR portals, staff are working from different versions of the same information. The result is double-booking, missed handoffs, and chronic phone calls to verify data that should already be visible in the system.
Manual Coordination and Phone-Tag Culture
Each phone call in a scheduling workflow is a potential point of failure. An unanswered call pushes a conflict downstream. A voicemail delays confirmation by an hour. Sequential outreach to multiple vendors — a standard practice in transport coordination — turns a single missed call into a cascade of delays.
VectorCare's own operational data shows traditional NEMT coordination takes an average of 31 minutes per request when managed manually. Across dozens of daily requests, that overhead accumulates fast.
Inadequate Staffing Forecasts
The Bureau of Labor Statistics projects approximately 189,100 RN openings per year through 2034. With that level of workforce pressure, scheduling built on static templates — rather than real-time or predictive demand — will consistently fail to absorb volume surges and unexpected absences.
Poor Cross-Organizational Communication
Healthcare scheduling spans multiple organizations: nursing units, transport providers, receiving facilities, home health agencies, DME suppliers. Without shared visibility or standardized protocols, every handoff is a blind transfer — one party assumes the next has confirmed, and no one catches the gap until a patient is already waiting.
Lack of Contingency Planning
Patient conditions change. Staff call out. Vehicles break down. Organizations without built-in buffers, on-call protocols, or flexible vendor networks have no structural capacity to absorb these disruptions. When contingency planning is absent, every unexpected event creates a visible failure — and usually a delayed patient.
Proactive Strategies to Prevent Healthcare Scheduling Conflicts
Most scheduling conflicts don't emerge from bad decisions — they emerge from infrastructure gaps: fragmented visibility, manual handoffs, and processes that have no fallback when something breaks. These five strategies address the structural causes.
Centralize Scheduling Visibility Across All Stakeholders
Moving from fragmented, departmental scheduling views to a unified environment gives every relevant stakeholder — transport coordinators, bed managers, clinical staff — a shared picture of what's happening in real time.
Ochsner Health's centralized patient flow center shows what this enables at scale: the system eliminated approximately 5,000 calls per month and attributed an estimated 56 lives saved annually to improved coordination visibility.
Practical starting point: Audit your current scheduling ecosystem. Count how many separate tools or channels hold scheduling-relevant information — phone logs, fax queues, individual EHR portals, spreadsheets. Each one is a visibility gap. Prioritize consolidation around a platform that displays:
- Patient transport status in real time
- Bed availability and discharge readiness
- Staff availability across shifts
- Vendor response and confirmation status
Automate Coordination to Eliminate Manual Bottlenecks
Every step that requires a human to initiate, confirm, or relay information is a step where the process can stall. Manual coordination doesn't just slow things down — it creates the conditions for conflict.
The highest-failure-risk steps are predictable: matching transport resources, broadcasting requests to multiple providers, and tracking confirmations without phone calls. Automation targets all three.
VectorCare's A.D.I. (Automated Dispatching Intelligence) demonstrates what this looks like at operational scale. The platform processes a new request every 23 seconds, simultaneously broadcasts to the full contracted vendor network rather than calling providers sequentially, and automatically selects the optimal vendor based on configurable criteria — ETA, cost, or preferred-vendor relationships. In 2025, A.D.I. saved healthcare systems and suppliers more than 100,000 hours of administrative time.
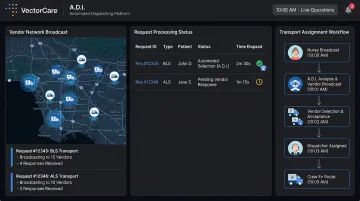
EHR integration extends these gains further. VectorCare's SMART on FHIR connection with Epic automatically pulls patient vitals, weight, and clinical data into the transport request — eliminating manual transcription, a common source of entry errors and scheduling mismatches.
Standardize Communication Protocols and Escalation Pathways
Without defined protocols, staff default to informal workarounds that vary by individual, shift, and department. That inconsistency creates invisible gaps: a conflict caught on one shift goes unresolved on the next because there's no standard process for raising it.
Build a tiered escalation structure:
- Tier 1 — Staff-level resolution within a defined window (e.g., 30 minutes)
- Tier 2 — Supervisor intervention when Tier 1 fails or when patient safety is in question
- Tier 3 — Administrative override for urgent patient care cases
Document these pathways. Make them accessible on every shift.
Build Flexible Capacity: Buffers, Float Pools, and Backup Providers
Scrambling when something breaks costs more and resolves worse than building flexibility into the schedule before it's needed.
Design for disruption:
- Buffer time between patient transports or procedures to absorb delays without cascading
- Float staff pools sized to absorb unplanned absences without leaving coverage gaps
- Pre-vetted backup transport providers, credentialed and contracted, ready to deploy without fresh vetting during a crisis
Engage Staff in the Scheduling Process
Staff who feel heard flag potential conflicts early. Those who don't tend to absorb them silently until they become visible failures.
Gather regular input on recurring pain points, workload patterns, and shift preferences. Where operationally feasible, implement self-scheduling or shift-swap tools that give clinical staff agency while maintaining coverage requirements.
How to Resolve Healthcare Scheduling Conflicts When They Occur
Even well-designed systems face conflicts. A structured resolution process protects patient care continuity when they do.
Triage and Prioritize by Patient Care Urgency
Not all conflicts carry equal consequence. The first question in any conflict response should be: "What is the impact on patient care?"
Use a three-tier framework:
- High urgency — Time-sensitive transport or care transition; immediate resolution required
- Moderate — Operational disruption without immediate safety risk; resolve within hours
- Low — Administrative overlap that can be resolved without escalation
Prioritize resolution resources by tier, not by who raised the issue first.
Communicate Transparently — Before You Have a Resolution
As soon as a conflict is identified, notify all affected stakeholders: the patient or family, the receiving facility, transport providers, and the clinical team. Early notification gives all parties time to prepare contingencies — waiting until you have a solution forces reactive scrambling that creates secondary conflicts. Provide staff with standardized communication templates to reduce variation across shifts.
Apply Structured Resolution in Order
Work through resolution options sequentially:
- Adjust — Find a mutually workable time or resource within the existing schedule
- Reallocate — Assign an available staff member, alternate provider, or substitute resource
- Defer — Shift lower-priority tasks to free capacity for the urgent need
- Escalate — Engage leadership only when the above options are exhausted
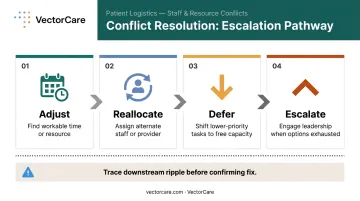
One caution: sequence changes carefully. A resolution that fixes one conflict by overloading a downstream resource creates the next conflict. Trace the ripple before confirming the fix.
Document Every Conflict for Future Learning
Every resolved conflict contains diagnostic information. Build a lightweight conflict log that captures:
- Type of conflict and root cause
- Resolution applied
- Time from identification to resolution
- Recurrence flag (has this happened before?)
StatPearls' healthcare conflict management guidance recommends documenting agreements and establishing contingencies as standard resolution steps. That documentation is what prevents the same conflict from recurring.
Building a Culture of Continuous Scheduling Improvement
Resolving individual conflicts matters — but building systems that prevent them is what reduces their frequency over time.
Establish Regular Scheduling Reviews
Weekly or biweekly huddles where scheduling managers review recent conflicts, near-misses, and emerging patterns shift the team from reactive to analytical. Patterns that repeat across multiple weeks point to systemic issues — not individual failures — and warrant structural changes rather than corrective coaching.
The Joint Commission requires that patient flow managers review measurement results to determine whether goals are being met and that leaders act on those results. That's the floor — high-performing teams build review cadences that go further, connecting scheduling data directly to operational decisions.
Track Meaningful KPIs
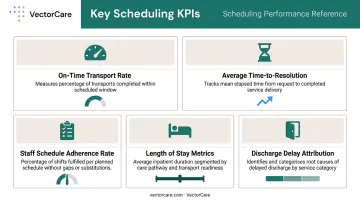
Focus on metrics that reflect scheduling health, not just activity volume:
- On-time transport rate — measures execution reliability
- Average time-to-resolution for scheduling conflicts — indicates process effectiveness
- Staff schedule adherence rate — reflects planning accuracy
- Length of stay metrics tied to discharge planning — connects scheduling performance to patient outcomes
- Discharge delay attribution — identifies which logistics factors are holding patients in beds
AHRQ's patient flow guidelines link ED crowding, boarding rates, and time-to-bed-assignment directly to hospital-wide scheduling effectiveness. These metrics belong on the same dashboard.
Invest in Conflict Resolution Training
Research on nursing conflict management identifies collaboration and accommodation as the most frequently effective styles in healthcare settings. StatPearls notes that while collaboration is the optimal win-win approach, it requires time — making compromise a practical necessity in time-pressured scheduling environments.
Training scheduling staff and clinical managers in structured communication, rapid prioritization, and collaborative problem-solving reduces the escalation rate of minor conflicts. Teams that practice these skills consistently are better equipped to contain major disruptions before they affect patient flow.
Frequently Asked Questions
How can I avoid scheduling conflicts in healthcare?
Avoiding conflicts requires centralizing scheduling visibility into a single platform, automating manual coordination tasks, and standardizing communication and escalation protocols. The goal is making conflicts visible and addressable before they reach patients — which requires infrastructure changes, not just process adjustments.
How do I resolve a scheduling conflict in healthcare?
Triage by patient care urgency first, then notify all affected stakeholders immediately — before you have a resolution. Work through adjustment, reallocation, and deferral options in order, escalate only when needed, and document the resolution to prevent recurrence.
What are the most common causes of scheduling conflicts in healthcare?
The leading causes are siloed scheduling systems with no shared visibility, reliance on manual phone-based coordination, inadequate demand forecasting, poor cross-organizational communication between nursing units and external providers, and no contingency capacity for last-minute disruptions.
What are the 5 C's of conflict resolution?
The 5 C's framework (Clarify, Communicate, Collaborate, Compromise, Choose) provides a structured path through disagreement. In healthcare scheduling, each step maps directly to practice: clarify the patient care impact, communicate with all affected parties, collaborate on workable options, compromise when time demands it, and choose the resolution that minimizes downstream disruption.
What is the 5-5-5 method of conflict resolution?
The 5-5-5 method gives each party five minutes to present their perspective, five minutes to respond, and five minutes jointly to identify a solution — a format well-suited to time-pressured healthcare settings where extended negotiation isn't an option.
How does technology help reduce healthcare scheduling conflicts?
Modern scheduling platforms reduce conflicts by automating resource matching, providing real-time visibility across all stakeholders, and integrating with EHR systems to eliminate manual data entry errors. Platforms like VectorCare go further — automating dispatching across contracted vendor networks and surfacing conflicts before they affect care delivery.