Introduction
A nurse completes a discharge assessment. A transport coordinator reaches for the phone. A care manager opens a second system to fax the DME order. A home health referral goes out by mail.
This is healthcare in 2025 — and it costs more than anyone realizes. CAQH found $89 billion spent on tracked administrative transactions, with $18.3 billion in potential savings available through full electronic adoption. Meanwhile, physicians average 7.9 hours weekly on administrative tasks alone, with documentation burden actively crowding out access to outside patient records.
Healthcare integration is the infrastructure-level answer — the connective layer that determines whether a discharge order automatically triggers a transport request or kicks off another round of phone tag. This article defines healthcare integration, breaks down the four primary integration types, and provides a practical framework for selecting the right approach for your organization's systems, scale, and compliance requirements.
Key Takeaways:
- Healthcare integration connects clinical and operational systems so data flows automatically — eliminating manual re-entry and communication delays
- Four integration types exist, ranging from simple point-to-point connections to unified coordination platforms
- ONC data shows 71% of non-federal acute care hospitals now enable patient access via FHIR APIs — signaling the regulatory direction of travel
- Choosing the right type depends on system count, IT capacity, compliance needs, and scale
- The right approach addresses coordination failures, not just data movement
What Is Healthcare Integration?
Healthcare integration is the technical and operational process of connecting two or more health systems — clinical, administrative, or logistical — so that data moves automatically, accurately, and in compliance with privacy standards like HIPAA.
In practice, that means:
- An EHR sending patient demographics directly to a transport platform when a discharge order is placed
- Lab results routing to a physician's dashboard without a phone call
- A home health agency receiving referral data at the moment of hospital discharge
- DME orders transmitting electronically to vendors rather than via fax
Integration is not a software feature. It's infrastructure: the same way roads connect cities, integration connects the systems healthcare runs on. Without it, even well-designed individual systems become information dead ends that staff must manually bridge, one phone call at a time.
What Integration Looks Like in Patient Logistics
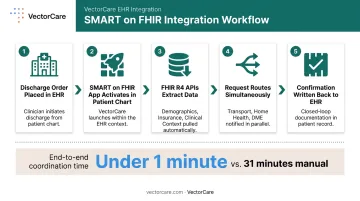
VectorCare's platform illustrates this infrastructure role clearly. When a discharge order is placed in Epic, the platform's SMART on FHIR app activates within the patient's chart, automatically pulling demographics, insurance, pickup location, and clinical context via FHIR R4 APIs. What previously took 31 minutes of phone-and-fax coordination compresses to under one minute.
That same request simultaneously routes to transport, home health, and DME workflows, all from within the clinical environment, without the coordinator switching systems. The result is a single trigger point replacing what used to be a chain of manual handoffs.
Why Healthcare Integration Matters in Modern Care Delivery
Fragmented systems create predictable failures. The mechanisms differ, but the outcomes cluster around the same categories: delayed decisions, duplicated effort, safety events at handoffs, and staff capacity consumed by coordination instead of care.
The Operational Cost of Disconnection
Without integration, these failures are structural — not individual:
- Delayed discharges because transport can't confirm availability and the EHR doesn't communicate with the scheduling platform
- Duplicated patient intake when systems don't share demographics across care settings
- Missed medication reconciliation because the specialist's notes never reached the primary EHR
- Care transitions running entirely on fax: no status tracking, no confirmation, no audit trail
A 2024 AHRQ report found medication list discrepancies in 35.4% of prescriptions during care transitions, with 9.7% classified as potentially harmful. That's not an outlier — it's what happens when handoff workflows rely on manual communication between disconnected systems.
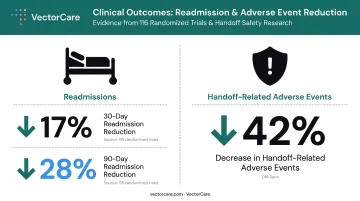
The Outcome Case for Integration
The strongest argument for integration investment isn't efficiency — it's clinical outcomes.
A 2025 systematic review and meta-analysis of 116 randomized trials published in JAMA Network Open found EHR-based interventions associated with 17% lower 30-day all-cause readmissions and 28% lower 90-day readmissions. The same AHRQ analysis found that structured, integrated handoff programs produced a 42% decrease in handoff-related adverse events.
Fragmentation reliably undermines these outcomes. When data exchange is treated as a back-office IT function, the cost surfaces elsewhere — in readmissions, preventable adverse events, and care transitions that depend on phone calls and faxes to close the loop.
The Four Types of Healthcare Integration
Healthcare integration is not one-size-fits-all. The right approach depends on how many systems need to connect, how complex the data is, what technical resources are available, and how much the organization needs to scale.
These four types represent a spectrum — from targeted and simple to comprehensive and coordinated. Most organizations use more than one simultaneously across different workflows.
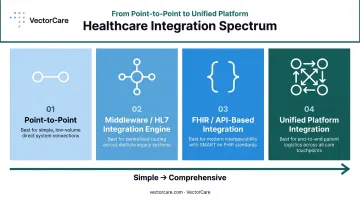
Point-to-Point Integration
What it is: A direct connection between two specific systems, custom-built to share a defined dataset — for example, an EHR sending ADT (admission/discharge/transfer) notifications to a scheduling platform.
How it works: One system sends a message triggered by an event; the receiving system is configured to accept and act on it. No intermediary layer exists.
Best suited for: Small organizations with few systems to connect, or a single high-priority integration where scope is clearly defined and budget is constrained.
Strengths:
- Fast to implement for a narrow use case
- Low initial cost
- Minimal infrastructure overhead
- Easy to test and validate
Limitations:
- Doesn't scale — each new system requires an entirely new custom connection
- Creates a fragile web of dependencies as the system count grows
- ONC data shows 54% of hospitals cited custom interface development as a barrier to electronic information sharing, and 72% reported challenges exchanging across different vendor platforms
Point-to-point works for narrow, stable workflows. Treated as a default architecture, it creates technical debt that compounds with every new system added.
Middleware / Integration Engine (HL7-Based)
What it is: A central integration engine — sometimes called a message broker or interface engine — that routes, translates, and distributes messages between multiple systems using health data standards, most commonly HL7 v2. Tools like Mirth Connect operate on this model.
How it works: The engine sits between systems, receives data from a source, transforms it into the format the destination system expects, and routes it to the correct endpoint — enabling many-to-many communication from a single hub.
Best suited for: Mid-to-large organizations running multiple systems that share data across departments — labs, pharmacies, radiology, EHRs, billing — where HL7 v2 message types (ADT, ORU, ORM) are already embedded in the ecosystem.
Strengths:
- Highly effective for high-volume transactional data like lab results, orders, and patient demographics
- Reusable interface templates reduce build time for subsequent connections
- HL7 v2 is used in over 90% of American hospitals and remains deeply embedded in core operational messaging
Limitations:
- HL7 v2 lacks semantic interoperability — systems can exchange data without sharing its meaning
- Middleware platforms require ongoing technical expertise to manage and update as systems evolve
- HL7 v2 isn't disappearing, but new use cases are increasingly built on FHIR rather than legacy messaging standards
For most organizations, the practical question is which workflows require message reliability versus real-time API access. Running HL7 and FHIR in parallel is common — and often the right answer.
FHIR / API-Based Integration
What it is: FHIR (Fast Healthcare Interoperability Resources) is the ONC-mandated standard for healthcare data exchange via RESTful APIs. FHIR-based integration allows systems to share structured, semantically consistent data through lightweight API calls, using the same general model that consumer applications use to share data.
How it works: Each system exposes FHIR-compliant API endpoints. Authorized applications request or push specific data resources — Patient, Encounter, Observation, Appointment — in real time. SMART on FHIR extends this by embedding apps directly inside EHR environments like Epic.
Best suited for: Organizations building new digital health applications, vendors integrating with EHR ecosystems, and any environment where real-time data access and cross-organizational interoperability are required. Increasingly mandated by payers and federal programs.
Why it's the regulatory direction of travel: ONC's 21st Century Cures Act Final Rule and CMS-9115-F both established information-blocking prohibitions and API access requirements. Hospital use of FHIR APIs for patient access grew from 57% in 2021 to 71% in 2024 — a 14-percentage-point increase in three years.
A concrete example: VectorCare's SMART on FHIR integration with Epic automatically extracts patient demographics, insurance information, pickup location, and clinical context the moment a transfer request is initiated — eliminating manual data entry and enabling simultaneous broadcast to multiple transport providers within seconds.
Limitations:
- Implementation depth varies significantly across EHR vendors
- Legacy systems may require bridging solutions
- Initial development investment is significant without pre-built integration tooling
- Many FHIR apps remain outside major EHR galleries due to maturity gaps or listing costs
VectorCare's SoFaaS™ (SMART on FHIR as a Service) platform addresses this barrier directly, enabling healthcare vendors to build and deploy EHR-embedded FHIR applications in weeks rather than years — without requiring internal FHIR expertise.
Unified Platform Integration
What it is: A unified platform consolidates routing, data exchange, workflow automation, and cross-party coordination into a single purpose-built environment designed for a specific operational domain. Rather than just moving data, the platform acts on it.
How it works: The platform integrates with upstream systems (EHRs, payer tools, scheduling software) via APIs or HL7, then manages the end-to-end workflow within its own environment — dispatching, tracking, communicating, and closing the loop. Users don't toggle between systems because the coordination happens inside the platform.
Best suited for: Health systems managing complex, multi-party workflows where coordination — not just data exchange — is the core challenge. Transfer centers, discharge planning teams, and care transition coordinators managing transport, home health, and DME simultaneously.
How VectorCare operates on this model: When a discharge order is placed in Epic, VectorCare's platform handles the complete downstream workflow: transport dispatch via ADI (Automated Dispatching Intelligence), home health referral, DME coordination, real-time tracking written back to the EHR, proof-of-service capture, and electronic billing — all from within the clinical environment, across a single connected platform. Orange County Health Care Agency reduced service request processing from 45 minutes to 4.5 minutes using this model.
Strengths:
- Eliminates coordination overhead that pure data-integration approaches leave behind
- Enables automation — automated dispatching, simultaneous multi-provider broadcast, real-time status updates
- Reduces manual phone calls, faxes, and follow-up loops across all parties
Limitations:
- Purpose-built platforms are domain-specific and don't replace underlying data integration standards
- Requires organizational commitment to workflow change and staff adoption
- Effectiveness depends on how many service providers and facilities are already networked within the platform
How to Choose the Right Healthcare Integration Strategy
The right integration type is determined by operational reality — not by what's most technically sophisticated. Start with needs.
| Factor | Points Toward |
|---|---|
| Two systems, one data type | Point-to-point |
| 5+ systems sharing structured clinical data | Middleware or FHIR |
| New app development or Epic integration | FHIR / SMART on FHIR |
| Multi-party coordination across transport, home health, DME | Unified platform |
| Legacy HL7 environment, high message volume | Middleware (HL7) |
| Regulatory alignment with ONC/CMS | FHIR-based |
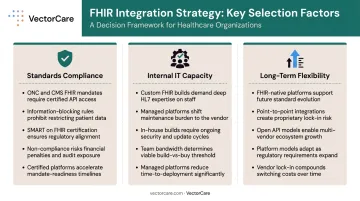
Three factors consistently separate good integration decisions from ones organizations regret:
- Standards compliance: ONC's information-blocking rules and CMS interoperability mandates are pushing the industry toward FHIR. Any organization choosing an integration approach today should factor in the compliance cost of proprietary or legacy-only lock-in.
- Internal IT capacity: Assess honestly whether your team can build and maintain custom integrations, or whether a managed platform with vendor support is more realistic. No-code platforms lower that barrier — VectorCare's Hub module, for example, enables workflow configuration without engineering-intensive custom development.
- Long-term flexibility: FHIR-based and platform integration models accommodate new systems, data types, and standards without requiring full rebuilds. Point-to-point webs rarely do.
What to Check Before Finalizing Your Integration Approach
The wrong integration choice doesn't just slow implementation — it creates compliance gaps and technical debt that compound over time. Before committing, run through these three checks:
- Start with the actual use case, not the ideal architecture. Many organizations build complexity into initial integrations and then under-resource the ongoing maintenance — match the solution to what you need now, not a theoretical future state.
- Compliance must hold at the integration layer, not just the endpoints. API security, encryption standards, access controls, and audit trails each need to meet HIPAA requirements independently — confirm any vendor can sign a Business Associate Agreement (BAA) before the conversation goes further.
- Don't let existing vendor relationships drive the decision. As FHIR adoption accelerates and federal mandates tighten, organizations locking into proprietary or legacy-only approaches today will face costly re-integration within the next budget cycle.
Frequently Asked Questions
What is healthcare integration?
Healthcare integration is the process of connecting disparate clinical, administrative, and operational systems so data flows automatically between them. It eliminates manual re-entry, reduces errors, and enables coordinated care across the continuum: from EHRs to transport platforms to billing tools.
What is a healthcare integrator?
A healthcare integrator is a technology vendor, consultant, or platform that builds and maintains the connections between health systems — translating data between formats, managing routing, and ensuring compliant, secure data exchange. VectorCare functions as a managed integrator, deploying and maintaining the integration layer on behalf of health system partners.
What are examples of integrated care?
Common examples include:
- An EHR automatically populating a transport request when a discharge order is placed
- A lab result routing directly to a physician's dashboard without a phone call
- A home health agency receiving patient demographics from a hospital at the point of referral
- A DME order transmitting electronically with proof-of-delivery written back to the patient chart
What are the 4 levels of interoperability in healthcare?
HIMSS defines four levels: foundational (data can be sent and received), structural (data format is standardized), semantic (shared meaning across systems), and organizational (policies and governance enable cross-organizational data use).
What is the difference between healthcare integration and interoperability?
Integration is the technical act of connecting specific systems to exchange data. Interoperability is the broader capability for those systems to exchange and meaningfully use information. Integration enables interoperability, but achieving it also requires shared standards, governance, and organizational alignment.
How does FHIR support healthcare integration?
FHIR provides a standardized RESTful API framework that gives health systems a common language for data exchange. Integrations built on FHIR deploy faster, scale across EHRs without custom-building each connection, and extend further through SMART on FHIR, which enables app deployment directly inside EHR workflows.