Introduction
Healthcare organizations are managing a financial environment that grows more complex each year. Rising patient volumes, multi-payer insurance structures, and a steady shift of costs onto patients have turned payment processing into a frontline operational priority — not a back-office afterthought.
The scale reflects the stakes. The U.S. healthcare digital payment market reached $3.98 billion in 2024 and is projected to hit $26.83 billion by 2034 — a growth rate that leaves no room for outdated revenue cycle infrastructure.
This article breaks down how healthcare payment processing works, what's driving revenue leakage, and how operational decisions — including patient logistics — affect billing accuracy.
What Makes Healthcare Payment Processing Unique
Multiple Payers, One Transaction
Retail payments involve one buyer, one seller, one transaction. A single patient encounter can involve the patient, a primary insurer, a secondary insurer, Medicare or Medicaid, and an employer health plan — each with different coverage rules, billing codes, and reimbursement timelines. Billing staff must reconcile all of them, in sequence, before collecting a dollar.
Dual Compliance Requirements
Payment platforms in healthcare don't just need to satisfy financial regulations. They operate under two overlapping compliance frameworks simultaneously:
- PCI-DSS — governs any system that stores or processes credit card payment data
- HIPAA — governs the privacy and security of protected health information (PHI), including financial data tied to patient records
Any vendor that touches patient billing data is typically required to sign a Business Associate Agreement (BAA), and security controls must satisfy both frameworks. A breach isn't just a financial penalty — it's a reputational event that erodes patient trust.
The Patient Responsibility Problem
With high-deductible health plans now covering 41.7% of privately insured individuals under 65, patients are bearing a larger share of costs than ever. U.S. out-of-pocket healthcare spending reached $556.6 billion in 2024 — equal to 11% of total national health expenditures.
That shift makes patient-facing collections a core revenue driver. More than one-third of covered workers are now enrolled in plans with deductibles of $2,000 or more for single coverage. If a provider can't collect from patients effectively, the financial gap doesn't close itself.
Legacy Infrastructure and the Expectation Gap
The technology gap is real. 68% of payers still reimbursed providers by paper check in 2024, and 71% of providers report it takes more than 30 days to collect after a patient encounter. Meanwhile, 62% of consumers prefer to pay medical bills online.
When patients expect digital, self-service options and providers are still running paper-based workflows, collection rates drop and administrative costs climb. Closing that gap is as much a technology decision as an operational one.
How Healthcare Payment Processing Works: Step by Step
Healthcare payment processing follows a two-phase structure: insurance adjudication (what the payer owes) and patient billing (what remains after coverage). Both must happen accurately and in sequence for providers to recover full revenue.
Eligibility Verification and Pre-Authorization
The process starts before care is delivered. Staff verify a patient's coverage, confirm benefit details, and — for certain procedures — obtain prior authorization from the insurer.
This step is where errors are most costly. Registration and eligibility failures account for 22% of all claim denials, with coordination of benefits issues as the leading root cause. Front-end revenue cycle problems drive 41% of total denials. Every data error at intake compounds through the rest of the billing cycle.
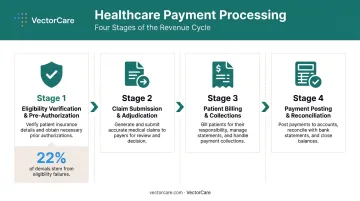
Claim Submission and Adjudication
Those front-end errors follow the claim downstream. After services are delivered, providers submit coded claims to payers — insurers or government programs — through clearinghouses that route and validate claims electronically. Medical claim submission has reached 97% electronic adoption, replacing the error-prone paper-based workflows that slowed reimbursement for decades.
The payer then adjudicates the claim: approving, partially paying, or denying it based on coverage terms and billing accuracy. Adjudication speed and accuracy vary significantly across payers, and the outcome directly determines how much and how quickly a provider gets paid.
Patient Billing and Collections
Once the insurer's payment posts, the remaining patient responsibility — copay, deductible, coinsurance — is billed directly to the patient. This step is increasingly digital: online portals, text-to-pay links, and installment plans.
The quality of this patient-facing experience matters. 32% of people would pay a medical bill within five minutes of receiving a text notification, yet only 16% had used a text-to-pay link in 2023. For providers, that gap represents recoverable revenue sitting in an underused channel.
Payment Posting and Reconciliation
This final step closes the loop — and it's where revenue leaks quietly accumulate if left unmanaged. Staff must:
- Match received payments to the correct patient accounts
- Reconcile remittances against expected reimbursement amounts
- Flag underpayments and discrepancies for follow-up
Done manually, each of these tasks is error-prone and slow. Modern revenue cycle management platforms automate matching and exception identification, cutting reconciliation time and improving financial accuracy across the board.
Common Healthcare Payment Methods
Healthcare providers typically accept a broader range of payment types than most industries, which matters because collection rates vary by patient population and balance size.
Primary payment methods include:
- Credit and debit cards — accepted in-person, online, and card-on-file for recurring charges
- Bank transfers / ACH — often preferred for larger balances; lower processing fees than cards
- Digital wallets (Apple Pay, Google Pay) — 64% of consumers use digital wallets for regular expenses, and adoption in healthcare is growing among younger patients
- HSA/FSA cards — important for patients in high-deductible plans, who make up a large and growing share of the patient population
Payment plans go beyond patient convenience — they're a direct revenue strategy. Many patients cannot pay large balances in a single transaction. Providers who offer structured installment plans, including automated recurring charges, see higher total collection and lower bad debt. Hospitals that require or encourage pre-service payment enrollment see 21% higher pre-service collections and 20% higher overall collection rates.
Payer-to-provider payments are also shifting. Electronic Funds Transfer (EFT) and Electronic Remittance Advice (ERA) are replacing paper checks and manual EOB reconciliation, improving both reimbursement speed and reconciliation accuracy. Yet with 68% of payers still issuing paper checks as of 2024, full automation in the payer-to-provider flow remains incomplete.
Key Challenges in Healthcare Payment Processing
Claim Denials
Denials are one of the most financially damaging problems in healthcare payment processing. Hospitals spent an estimated $19.7 billion in 2022 attempting to overturn denied claims — and more than 54% of those denied claims were ultimately overturned after multiple rounds of appeals. That's a massive investment of staff time and resources to recover revenue that should never have been lost.
The numbers reinforce the scale:
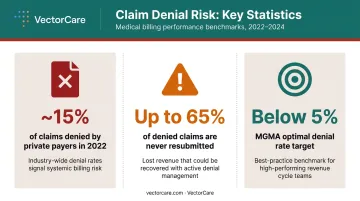
- Nearly 15% of claims submitted to private payers were initially denied in 2022
- Up to 65% of denied claims are never resubmitted by providers
- MGMA benchmarks set the optimal initial denial rate below 5% — most health systems are far above it
Manual and Fragmented Workflows
Claim denials don't happen in isolation — many trace back to the same root cause: disconnected systems. When billing platforms don't connect to EHRs, staff re-enter data by hand across multiple systems. That manual handoff creates duplicate errors, delayed submissions, and reconciliation headaches.
The downstream effects are measurable:
- MGMA benchmarks a clean claims rate target of 98% — fragmented workflows are a primary reason most systems fall short
- Charge capture should be completed within 3 to 5 days of service; manual processes routinely push that window out, slowing the entire revenue cycle
Patient Payment Collection
Providers collect only 24% of patient out-of-pocket billings owed after insurance — a figure that should alarm any CFO. Collection rates drop further as balances rise: for balances between $7,501 and $10,000, collection falls to 17%.
The underlying issues are communication failures and trust erosion. Only 22% of consumers knew their exact financial responsibility before a provider visit. Surprise billing compounds the problem — 65% of adults worry about unexpected medical bills, and that anxiety translates into payment avoidance.
Compliance and Security
Healthcare data breaches carry the highest average cost of any industry: $9.77 million per incident in 2024. When payment data and health records are combined in a single breach, the exposure is both legal and financial. Maintaining HIPAA compliance, PCI-DSS standards, and evolving state-level billing regulations requires continuous investment in both technology and staff training — and that investment never fully stops as regulations change.
Technology Innovations Shaping Healthcare Payment Processing
EHR Integration
When payment and billing systems connect directly to electronic health records via FHIR APIs, patient data flows automatically between clinical and financial systems. This eliminates manual re-entry at the point of claim creation — removing one of the most common sources of billing errors.
CMS's interoperability and prior authorization final rule (CMS-0057-F) is accelerating this shift. It requires impacted payers to implement FHIR-based prior authorization APIs, with decisions required within 72 hours for expedited requests and 7 calendar days for standard requests. CMS estimates the rule will save approximately $15 billion over 10 years.
AI and Denial Prevention
63% of healthcare organizations are already using AI and automation in the revenue cycle, according to an HFMA-FinThrive survey. The applications driving adoption include:
- Pre-submission claim scrubbing catches coding errors before claims go out
- Denial prioritization ranks appeals by likelihood of success, so staff focus where it pays off
- Prior authorization automation cuts the manual back-and-forth that delays approvals and inflates write-offs
Prior authorization had only 26% electronic adoption in 2022 — one of the largest remaining inefficiencies in the administrative cycle. AI-assisted automation is closing that gap faster than manual process improvement alone could.
Patient-Facing Technology
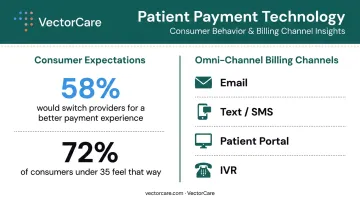
The same efficiency pressure showing up in back-end automation is also reshaping what patients expect at the point of billing. 58% of consumers say they would switch providers for a better payment experience, and 72% of consumers under 35 feel that way — making patient-facing technology a retention issue, not just a convenience one.
Omni-channel billing — email, text, portal, IVR — meets patients where they are. Pre-care enrollment technology goes further: letting patients review cost estimates and enroll in payment plans before receiving care, reducing the friction that makes post-service collection so difficult.
How Patient Logistics and Operational Efficiency Affect Payment Outcomes
The Connection Between Patient Flow and Billing Accuracy
How patients move through a care setting directly shapes how accurately — and quickly — that care gets billed.
When patient transfers, discharges, and care coordination are delayed or poorly documented, billing suffers downstream. Incomplete information at handoff leads to:
- Coding errors from missing clinical context
- Delayed claim submission due to unresolved discharge documentation
- Extended length of stay (LOS) costs that complicate both DRG-based billing and patient responsibility calculations
Nearly 30% of older individuals experience hospital discharge delays, and patients waiting in the emergency department for more than a day before admission tend to have longer overall stays. Those extended stays carry real cost — mean hospitalization costs for excessively prolonged stays run nearly three times higher than standard cases.
Automating Care Coordination to Protect Billing Integrity
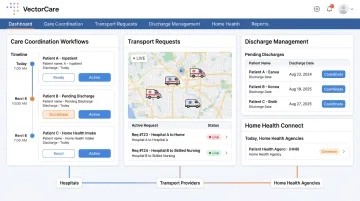
Reducing administrative burden in care coordination creates cleaner handoffs, which support accurate, timely billing. When scheduling, transport requests, and discharge workflows are automated rather than managed through phone calls and manual entry, the documentation record is more complete and the time from discharge to claim submission is shorter.
VectorCare's patient logistics platform is designed specifically for this operational layer. By automating coordination across hospitals, transport providers, and home health agencies, it reduces the fragmented communication that precedes billing errors. VectorCare's ADI (Automated Dispatching Intelligence) saved healthcare systems more than 100,000 hours of administrative work by 2025 — hours that previously went into manual coordination tasks, delaying care transitions and the documentation those transitions generate.
EHR Integration and the Documentation Record
VectorCare's SMART on FHIR integration with Epic means that care transition data — transport requests, discharge triggers, provider assignments — flows directly from the EHR into the logistics workflow without manual re-entry. This eliminates the data handoff gaps where billing errors most often originate.
When every logistics event is tied to a structured, EHR-anchored record, the documentation available for claim substantiation is more complete. That completeness supports LOS accuracy, dispute resolution, and a faster revenue cycle from discharge through payment posting.
Frequently Asked Questions
What are the steps in healthcare payment processing?
The core sequence runs: eligibility verification and pre-authorization before care is delivered, claim submission and adjudication after services are rendered, patient billing for the remaining balance once the insurer pays, and payment posting and reconciliation to close the cycle. Each step must flow accurately into the next or downstream revenue is at risk.
What are the payment methods for healthcare?
Providers typically accept credit and debit cards (in-person, online, and card-on-file), bank transfers and ACH, digital wallets such as Apple Pay and Google Pay, HSA/FSA cards, and structured payment plans. Offering multiple options directly improves collection rates, since patient populations vary widely in how they prefer to pay.
What compliance requirements apply to healthcare payment processing?
Two frameworks govern simultaneously: HIPAA covers patient health and financial data privacy, while PCI-DSS applies to any system storing or processing card payments. Vendors with patient data access must sign Business Associate Agreements (BAAs), and staying current with both frameworks — plus evolving state-level billing rules — requires ongoing compliance investment.
How does extended patient length of stay affect healthcare billing and payment?
Delays in discharge or patient transfer extend inpatient stays, increasing costs and complicating DRG-based billing, which reimburses at predetermined rates regardless of actual service volume. Extended stays also create administrative backlogs — incomplete documentation at discharge delays claim submission and slows the entire payment cycle.
How is AI changing healthcare payment processing?
AI is being applied primarily to denial prevention, prior authorization automation, and predictive analytics that help billing teams prioritize which denied claims are worth appealing. Human oversight remains essential for complex edge cases, but AI is shifting the revenue cycle from reactive to preventive.