The distinction matters more now than ever. With the Medicare Shared Savings Program covering more than 10.8 million beneficiaries across 480 ACOs in 2024 and generating $2.4 billion in net savings, value-based care models are forcing health systems to draw sharper lines between what counts as a structured program and what counts as a workflow activity.
This article covers both: clear definitions, a side-by-side comparison, key distinctions across billing, scope, and credentialing requirements, and practical guidance on when to apply each.
Key Takeaways
- Care management is a structured, longitudinal program — formal enrollment, individualized care plans, ongoing monitoring — built for high-risk or chronically ill patients.
- Care coordination organizes information and handoffs across providers within a single episode; it is relational and process-focused, not a formal program.
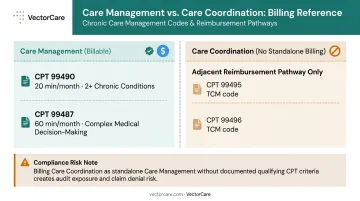
- Care management is billable under CMS CPT codes (99490, 99487); care coordination as a standalone function has no equivalent Part B billing structure.
- The two are complementary: effective care management always includes care coordination, but the reverse isn't true.
- Patient logistics — transport, discharge, transitions — sits beneath both functions and is the layer most likely to break down without dedicated infrastructure.
Care Management vs. Care Coordination: A Quick Comparison
| Attribute | Care Management | Care Coordination |
|---|---|---|
| Focus | Chronic disease management, outcomes | Information flow, handoffs, transitions |
| Time Horizon | Months to years (longitudinal) | Bounded episode or transaction |
| Patient Population | High-risk, 2+ chronic conditions | Any patient crossing care settings |
| Team Involvement | Multidisciplinary (physician, nurse, social worker, care manager) | Variable; often single coordinator role |
| Billing/Reimbursement | CPT 99490, 99487 (CMS CCM codes) | No standalone Part B billing code |
| Triggering Event | Enrollment criteria + risk stratification | Referral, discharge, or transition need |
| Key Output | Individualized care plan, outcome metrics | Structured handoff, information transfer |
| Setting | CCM programs, Medicaid MCOs, population health | Post-acute transitions, referral loops, medical homes |
In practice, the boundary between these two functions blurs regularly. The decision usually comes down to three factors: duration of engagement, whether CMS billing requirements apply, and whether a formal care plan must be maintained.
What Is Care Management?
AHRQ defines care management as a team-based, patient-centered approach designed to help patients and their support systems manage medical conditions more effectively. It emerged as a leading strategy for populations with chronic or complex conditions — not as a one-time intervention, but as a structured, iterative program.
The Care Management Cycle
Care management follows a defined process that repeats over time:
- Comprehensive needs assessment — clinical, behavioral, and social factors
- Individualized care plan development — documented, patient-centered, and living
- Implementation across disciplines — coordinated execution by a multidisciplinary team
- Ongoing monitoring — tracking adherence, clinical changes, and utilization
- Outcomes evaluation — measuring against defined metrics and adjusting the plan
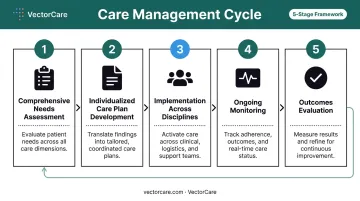
What distinguishes care management from a single clinical encounter is this cycle: it doesn't end at discharge — it continues until the patient's condition stabilizes or care goals shift.
Who Qualifies?
The eligible population is large. According to CDC data, 76.4% of U.S. adults — roughly 194 million people — have at least one chronic condition, and 4 in 10 have two or more. Among Medicare fee-for-service beneficiaries, approximately 75% have two or more chronic conditions, making them eligible for CMS Chronic Care Management programs.
CCM uptake remains low despite this scale. A 2024 study found enrollment among eligible Medicare beneficiaries rose only from 1.1% in 2015 to 3.4% in 2019 — a significant gap between the addressable population and actual participants.
CMS billing requirements (per MLN909188, revised June 2025):
- CPT 99490: Standard CCM — minimum 20 minutes of clinical staff time per calendar month, for patients with 2+ chronic conditions
- CPT 99487: Complex CCM — minimum 60 minutes per calendar month, requiring moderate or high complexity medical decision-making
Both codes require documented patient consent, 24/7 access to care, a comprehensive care plan, and continuity with a designated care team.
Care Management in Practice
Consider a patient with both diabetes and heart failure enrolled in a formal CCM program. A care manager conducts an initial comprehensive assessment, then builds a care plan covering medication management, dietary guidance, specialist coordination, and social support — including transportation to endocrinology and meal assistance.
Each month, the care manager reviews lab trends, adjusts the plan based on clinical changes, and logs time against CPT 99490. Over 12 months, the plan is updated multiple times — once after a hospitalization, again after a medication change.
Where care management is the primary function:
- Medicare CCM programs
- Medicaid managed care organizations
- Population health management programs
- Complex care programs for patients with 4+ chronic conditions or frequent hospitalizations
- PACE (Program of All-Inclusive Care for the Elderly) organizations
What Is Care Coordination?
AHRQ defines care coordination as the deliberate organization of patient care activities and sharing of information among all participants concerned with a patient's care to achieve safer and more effective care. The emphasis is on the word deliberate — coordination doesn't happen by default across fragmented systems. Someone has to own it.
Care coordination is relational and process-oriented. It focuses on information transfer, handoff quality, and alignment across providers, settings, or time points — not on longitudinal program management.
How Care Coordination Works
Care coordination typically operates through discrete, time-limited interactions:
- Identify the gap or transition need — a discharge, referral, or care gap
- Aggregate clinical information — history, medications, follow-up instructions
- Communicate via structured handoff — to the receiving provider or team
- Confirm receipt — close the loop with the receiving party
- Episode closes — no ongoing monitoring obligation
This is distinct from care management's sustained cycle. Coordination has a beginning and an end within a defined episode.
Who Benefits Most?
Care coordination applies broadly — to any patient whose care crosses providers or settings:
- Patients transitioning from hospital to rehabilitation or home
- Individuals in specialist referral loops where follow-through is unclear
- Children in pediatric medical home models requiring service linkages
- Any patient whose care spans multiple providers without formal program enrollment
Importantly, care coordination does not independently trigger a CMS care plan requirement, enrollment criteria, risk stratification, or formal outcome tracking. Those elements belong to care management.
Nearly 20% of patients experience adverse events within three weeks of discharge, according to AHRQ, with systematic care-transition failures at the root of most post-discharge harm. This makes transitions the highest-value target for structured coordination efforts — and the example below illustrates what that looks like in practice.
Care Coordination in Practice
A patient discharged after hip replacement surgery illustrates the model clearly. Before transport departs, the care coordinator:
- Assembles surgical notes, medication reconciliation, PT orders, and wound care instructions
- Contacts the receiving rehab team to confirm bed availability
- Sends clinical documentation via secure transfer
- Verifies the receiving nurse has everything needed
The coordination work is complete once the handoff is confirmed. No ongoing monitoring follows.
Primary settings:
- Post-acute transitions (hospital to SNF, SNF to home)
- Specialist referral loops
- Behavioral health integration within primary care
- Pediatric medical home models
Care Management vs. Care Coordination: Key Differences
Scope and Duration
Care coordination is bounded to an episode or transaction. Care management describes a sustained program that may span years.
Coordination is the bridge between two points; care management is the ongoing road. A coordinator hands a patient off and closes the episode. A care manager follows that patient through every subsequent clinical change, appointment, and setback.
Billing and Reimbursement
For health systems, billing is where this distinction has the most direct operational impact.
CMS has established specific CPT codes for care management:
- 99490: First 20 minutes of clinical staff CCM per calendar month
- 99487: First 60 minutes of complex CCM per calendar month, with moderate or high complexity medical decision making (MDM)
Both require eligible chronic conditions, documented consent, 24/7 access, a comprehensive care plan, and detailed time documentation.
Care coordination as a standalone function has no equivalent Part B billing structure. Coordination activities are reimbursed only when embedded in defined services — for example, Transitional Care Management (TCM) covers post-discharge management through CPT 99495 (face-to-face within 14 days) and 99496 (within 7 days). Labeling general coordination work as CCM without meeting CMS eligibility and documentation requirements creates compliance risk.
Care Plan Requirements
CMS mandates a comprehensive, patient-centered care plan for CCM enrollment, a living document updated in response to clinical changes. This is a program requirement, not optional documentation.
Care coordination may produce a care plan as a handoff tool (discharge instructions, referral summaries), but there is no obligation to maintain or update it over time. The handoff document is transactional; the CCM care plan is longitudinal.
Credentialing and Oversight
Formal care management programs are governed by accreditation standards. Two key frameworks apply:
- URAC offers case management accreditation at the program level
- CCMC's Board Certified Case Manager (CCM) credential requires a qualifying license or degree, plus documented experience across the full case management function: assess, plan, implement, coordinate, monitor, and evaluate
Care coordination performed as part of routine clinical workflow carries no equivalent credentialing requirement. A coordinator may organize handoffs and transfer information without holding a CCM credential.
When to Apply Each
| Situation | Apply This |
|---|---|
| Patient with 2+ chronic conditions needing monthly monitoring | Care management (CCM) |
| Patient being discharged from hospital to SNF | Care coordination |
| High-utilization patient requiring multidisciplinary team oversight | Care management |
| Specialist referral with unclear follow-through | Care coordination |
| Medicaid managed care enrollee with complex psychosocial needs | Care management |
| Post-surgical patient transitioning to home health | Care coordination |
How Care Management and Care Coordination Work Together
The two functions aren't competing — they're nested. Effective care management inherently includes care coordination. A care manager overseeing a patient's chronic disease program still has to coordinate across specialists, home health agencies, transport providers, and community supports to execute that plan. The coordination activities don't stop; they become part of a larger management structure.
What's often overlooked is the layer beneath both: patient logistics. Even the most well-designed care management program or structured handoff can fail if the patient doesn't physically get where they need to go. Transport to the follow-up appointment, timely discharge from the acute setting, reliable transfer to the rehab facility — these aren't administrative afterthoughts. They're the operational substrate that both functions depend on.
This is the problem VectorCare addresses. Its patient logistics platform automates the coordination layer that care teams currently manage through phone calls, faxes, and manual workflows. Care coordinators in manual environments spend an average of 31 minutes arranging a single non-emergency medical transport call — that overhead compounds across dozens of daily discharges.
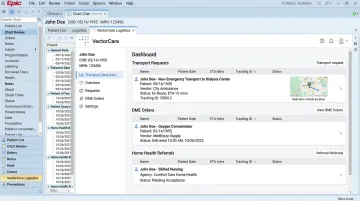
VectorCare's SMART on FHIR integration with Epic eliminates that burden by embedding transport requests, DME orders, and home health referrals directly into the clinical workflow. Patient data is auto-populated, and real-time vendor tracking is visible from within the EHR.
That evidence base matters for health systems evaluating where to invest. A 2022 systematic review found that non-emergency medical transportation interventions were associated with fewer missed appointments, and missed appointments are a primary driver of care coordination breakdown and readmission risk. Platforms that automate this layer deliver measurable returns:
- Reduce communication delays across care transitions
- Recover staff hours lost to manual transport scheduling
- Give care managers reliable execution beneath the plan they've built
- Lower readmission risk by closing the transport gap at discharge
Value-based contracts increasingly penalize avoidable readmissions and utilization — outcomes that depend as much on whether the patient got to the appointment as on the clinical plan itself. Health systems that treat logistics as infrastructure, not a scheduling function, are the ones building care management programs that actually hold together under that pressure.
Frequently Asked Questions
What is the difference between care management and care coordination?
Care coordination organizes information and handoffs across providers within a bounded episode — a discharge, a referral, a transition. Care management is a structured, longitudinal program with formal enrollment, documented care plans, and ongoing monitoring for high-risk or chronically ill patients — and unlike standalone care coordination, it is billable under CMS CPT codes.
What are the three C's of care coordination?
The three C's are commonly referenced as Communication, Collaboration, and Continuity. AHRQ's framework reinforces these by emphasizing clear accountability, organized information sharing, and consistent follow-up across all care participants.
What is the difference between a clinical care coordinator and a care manager?
A care coordinator manages information flow and transitions within a single episode — assembling documentation, confirming handoffs, closing referral loops. Care managers, often credentialed through the CCMC's CCM certification, take on a broader scope: long-term individualized care plans for complex patients, adjusted over time as clinical conditions change.
Can care management and care coordination be used together?
Yes, and they frequently are. Care management programs routinely incorporate care coordination activities — a care manager executing a chronic disease plan must also coordinate across specialists, home health, and transport providers.
Which conditions typically require care management rather than care coordination?
Patients with two or more chronic conditions, high utilization patterns (frequent ED visits or hospitalizations), or complex psychosocial needs are the primary candidates for formal care management. Care coordination applies more broadly — to any patient undergoing a transition, referral, or handoff, regardless of diagnosis complexity.
How does patient transport fit into care coordination?
When patients can't reach the next point of care on time, the coordination chain breaks — no matter how well the clinical handoff was structured. Missed rides, wrong vehicle types, and unconfirmed pickups are among the leading causes of coordination failures in post-discharge transitions to SNF or home health settings. Logistics platforms that automate transport scheduling and confirmation close this gap directly.