This guide is written for healthcare IT leaders and operations teams responsible for making AI API integrations work in production — not in theory. It covers interoperability standards, HIPAA compliance architecture, workflow design, and rollout strategy, with concrete examples from patient logistics environments where these principles have been pressure-tested at scale.
Key Takeaways
- Start with FHIR and SMART on FHIR — standards-first architecture cuts integration time significantly
- HIPAA compliance is the integration team's responsibility, not the vendor's
- Map workflows before writing integration code — define human handoff points explicitly
- Use a three-phase rollout: discovery, pilot, then scale
- Define measurable KPIs before go-live — vague success criteria derail even well-built integrations
Why Healthcare AI API Integration Is More Complex Than Standard Software Integration
Healthcare AI API integration connects AI-powered software to existing clinical infrastructure — EHRs, patient management platforms, transport coordination systems, payer databases — so data flows securely and intelligently between them.
The definition sounds simple. The execution isn't. Unlike standard API integration, healthcare AI APIs must handle protected health information (PHI), conform to strict regulatory standards, and often interact with legacy systems built on inconsistent data schemas.
Research published in the Annals of Internal Medicine found that ambulatory physicians spend nearly 49.2% of their office day on EHR and desk work — APIs are supposed to reduce this burden. A poorly designed integration does the opposite: it adds friction instead of removing it.
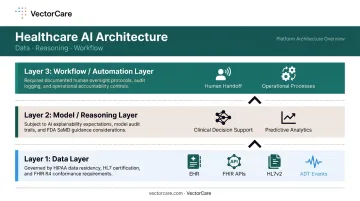
The Three Layers Every Healthcare AI Integration Team Must Understand
Healthcare AI API integration is not a single task. It's a layered architecture decision with three distinct components:
- Data layer: Pulls structured clinical data from EHRs and source systems using FHIR APIs, HL7v2 feeds, and ADT events
- Model/reasoning layer: The AI that processes that data and generates outputs such as clinical decision support, automated dispatching, or predictive analytics
- Workflow/automation layer: Delivers those outputs into operational processes with defined human handoff points
Each layer carries different compliance requirements and technical complexity. Teams that treat integration as a single endpoint connection, rather than a layered architecture, are the ones that end up with PHI in error logs, AI outputs nobody trusts, and workflows that clinical staff simply abandon.
Build on Proven Interoperability Standards: FHIR, HL7v2, and SMART on FHIR
The most consequential architectural decision in any healthcare AI integration is this: build on established interoperability standards. Proprietary data pipelines create maintenance debt, limit portability, and put you at odds with the direction the entire industry is moving.
FHIR (Fast Healthcare Interoperability Resources) is now the dominant standard for structured clinical data exchange. ONC reported that 69% of non-federal acute care hospitals used standards-based FHIR APIs for patient access in 2022 — up 12 percentage points from 2021. CMS has further anchored this trajectory by requiring impacted payers to implement HL7 FHIR Release 4.0.1 APIs by January 1, 2027. Integration teams should treat FHIR R4 as the baseline target.
What SMART on FHIR Actually Enables
SMART on FHIR (the HL7 SMART App Launch framework) allows third-party applications to launch directly within EHR environments using OAuth 2.0 authentication. When a clinician opens a SMART on FHIR app inside Epic, patient context is automatically populated: no manual data entry, no duplicate records, no context switching between systems.
This matters for workflow continuity. Clinicians who must leave their primary system to access an AI tool will either skip that tool or use it inconsistently. SMART on FHIR eliminates that friction by embedding AI-powered capabilities inside the EHR environment where clinical work actually happens.
FHIR Implementation Best Practices
Before writing integration code, do this groundwork:
- Standardize resource types first — agree on which FHIR resources you'll use (Patient, Encounter, Observation, ServiceRequest) and document how they map to your data model
- Test in a sandbox against real schema — validate all data mappings against representative patient records before touching production
- Plan for FHIR version differences across vendors — Epic, Oracle Cerner, and MEDITECH implement FHIR differently; assume variation and build to handle it
- Build a translation layer for HL7v2 — many hospitals still route ADT feeds and lab results over HL7v2; middleware that normalizes these into FHIR-compatible formats prevents the AI layer from having to interpret two incompatible standards simultaneously
How VectorCare Puts This Into Practice
Each of those implementation principles shows up directly in VectorCare's own stack. The VectorCare SMART on FHIR app — developed in partnership with Priority Dispatch Corp and listed on the Epic App Showroom — automatically extracts patient data directly from Epic, eliminating manual re-entry for patient logistics requests. A coordinator initiating a transport request gets patient demographics, clinical details, and discharge information auto-populated on submission.
In 2026, VectorCare launched SoFaaS (SMART on FHIR as a Service), which enables healthcare vendors to build, deploy, and scale EHR-embedded applications in weeks rather than months. The platform handles SMART on FHIR compliance, Epic certification, and health system installation, so partners focus on their domain expertise rather than integration infrastructure.
Make HIPAA Compliance and Data Security Non-Negotiable from Day One
HIPAA compliance cannot be bolted on after an integration is built. It must be architected into every layer from the start — before a single line of integration code is written.
This means governance documentation, vendor agreements, and technical controls must be in place before production deployment, not added during a post-launch audit.
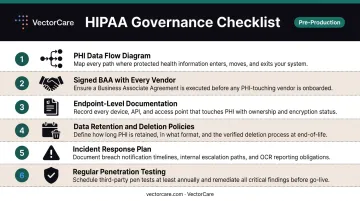
The Minimum Governance Checklist
Every healthcare AI API integration needs these six elements documented before production deployment:
- PHI data flow diagram — maps exactly where PHI enters, moves through, and exits the integration
- Signed BAA with every vendor — any third party that processes PHI requires a Business Associate Agreement
- Endpoint-level documentation — records what data is sent and received at each API call
- Data retention and deletion policies — defines how long PHI is held and how it's purged
- Incident response plan — specific to the API integration, not just the organization's general plan
- Regular penetration testing — covers integration endpoints, not just the application layer
The Compliance Gap Nobody Talks About
Here's where most teams get caught: they assume that using a HIPAA-compliant API vendor means their integration is automatically compliant. It is not.
A BAA covers what the vendor does with PHI, not what your integration does. PHI that appears in query parameters, gets logged in error messages, or gets cached in intermediate services creates violations even when the primary API vendor is fully certified.
OCR's 2023 enforcement activity documented exactly this exposure: MedEvolve paid $350,000 after a server misconfiguration left the PHI of 230,572 individuals accessible online. The server ran compliant software. The configuration did not.
Technical Controls Required
HHS guidance references NIST standards for encryption safe harbor: data at rest consistent with NIST SP 800-111, and data in motion consistent with NIST SP 800-52. Beyond encryption:
- Role-based access controls (RBAC) with minimum-necessary data access
- Audit logging of all API calls that touch PHI
- Automatic session timeouts for API-connected applications
Cloud infrastructure certifications (SOC 2, HITRUST) from your API vendor establish a baseline, but the integration architecture itself requires independent review. Vendor certification does not cover how your code handles, routes, or exposes PHI between systems.
AI Clinical Output Review
For AI APIs that produce clinical outputs — diagnoses, discharge summaries, treatment recommendations — best practice requires human review before any AI output reaches the patient record. Define in your integration design exactly where that review step happens, who owns it, and how it's documented in the audit trail.
Design Workflows for Automation, Validation, and Ongoing Governance
The biggest integration failures happen when AI APIs are connected to clinical systems without a workflow design. The API fires, data moves, but no one has defined what happens next, who owns edge cases, or how errors surface. Workflow mapping must precede integration architecture. Build the process map first; the technical layer follows it.
Testing and Validation Framework
Run integration validation in three stages:
- Synthetic data in sandbox — verify API behavior, data mapping, and error handling without touching real patient records
- De-identified historical records — test AI output quality against representative clinical data; define what "acceptable" looks like before this stage begins
- Parallel production testing — run old and new workflows simultaneously before full cutover; the success criterion is not "does the API respond" but "does the AI output match expected standards in at least X% of cases"
Define those X% thresholds before testing starts. Teams that don't set explicit quality criteria end up in endless subjective debates about whether the integration is "good enough."
Ongoing Governance
Healthcare AI integrations are not set-and-forget systems. FDA guidance notes that AI system performance can be affected by changes in clinical practice, patient demographics, data inputs, and infrastructure — a phenomenon known as model drift.
Assign explicit ownership for:
- Integration monitoring — who watches API uptime, error rates, and data quality
- AI output review — who evaluates whether model accuracy is degrading over time
- Escalation path — what happens when the AI produces a problematic output in production
VectorCare's A.D.I.: Workflow-First AI Design in Practice
VectorCare's Automated Dispatching Intelligence (A.D.I.) illustrates what happens when AI integration is designed around existing workflows rather than bolted onto them after the fact. The system processes a new transport request every 23 seconds and sends broadcasts every 12 seconds across a network of 2,500+ healthcare facilities. In 2025, A.D.I. saved healthcare systems over 100,000 hours by eliminating repetitive coordination tasks — automating the mechanical steps that consumed dispatcher time while keeping human judgment where it belongs. The result: a 90% reduction in manual coordination.

That outcome was only achievable because the automation was designed around the existing dispatch process. Every human handoff point was mapped before a single line of automation was written — which meant the system supported dispatchers from day one instead of creating new friction for them to work around.
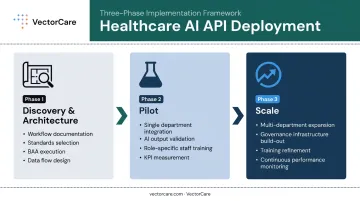
Phased Implementation: How to Roll Out Healthcare AI APIs Without Disrupting Care
A three-phase rollout approach outperforms big-bang deployments in healthcare AI integration.
The Three Phases
Phase 1 — Discovery and Architecture
- Document current state workflows end-to-end
- Select interoperability standards and confirm FHIR version targets
- Execute BAAs with all vendors
- Design the full data flow diagram before writing code
Phase 2 — Pilot
- Integrate with one department or use case only
- Validate AI outputs against baseline performance
- Train staff on the new workflow (role-specific, not generic)
- Measure against defined KPIs before proceeding
Phase 3 — Scale
- Expand to additional departments or use cases based on pilot learnings
- Build on the governance and monitoring infrastructure established in Phase 2
- Refine and redeploy training materials developed during the pilot
Staff Training and Change Management
Clinician resistance, not technical failure, is the leading cause of healthcare technology adoption failure. A JAMIA Open scoping review found that EHR training programs designed specifically for clinical practice had favorable training-related outcomes, while generic training did not perform as well.
Training must be role-specific. What changes for a nurse differs from what changes for a care coordinator or a transfer center specialist. Include clinical champions in workflow design from the start as active participants — they will identify failure modes that IT teams simply won't see.
Define "Done" Before You Start
Set measurable KPIs before the pilot begins:
- Reduction in manual data entry minutes per shift
- Time-to-transport request completion
- Error rate in patient record matching
- Staff hours saved per month
Without a baseline and defined success criteria, go/no-go decisions on scaling rest on gut feeling. Executives need specific metrics — reduction percentages, time saved, error rates — to justify expanding an integration beyond the pilot department.
Common Healthcare AI API Integration Mistakes and How to Avoid Them
Mistake 1: Skipping the Sandbox
Teams under deadline pressure push integrations directly to production. In healthcare, a data mapping error can route the wrong patient information to the wrong clinician or delay a time-sensitive transport request.
Mandate a defined sandbox-to-production pathway with documented sign-off gates. No exceptions.
Mistake 2: Treating Compliance as the Vendor's Problem
A signed BAA does not mean an integration is HIPAA-compliant. Integration teams must own the full PHI data flow diagram and conduct their own security review.
The MedEvolve and iHealth Solutions OCR settlements are both documented examples of organizations that had compliant vendors but misconfigured integrations. Vendor compliance covers the vendor's infrastructure — not yours.
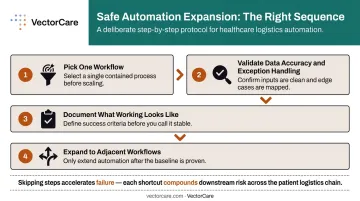
Mistake 3: Over-Automating Too Early
Connecting AI APIs across multiple workflows before any single one is validated creates cascading failures. Start narrow, prove the model, then expand.
A practical sequence:
- Pick one workflow (for example, transport dispatching or discharge scheduling)
- Validate data accuracy and exception handling in that workflow alone
- Document what "working" looks like before touching the next integration
- Only then expand to adjacent workflows
Frequently Asked Questions
What is healthcare AI API integration?
Healthcare AI API integration is the process of connecting AI-powered tools to existing clinical systems — EHRs, transport platforms, payer databases — using standardized protocols. It enables automation, data exchange, and AI-driven decision support while maintaining HIPAA compliance throughout the data flow.
What compliance requirements apply to healthcare AI API integrations?
HIPAA compliance covers four core requirements for any vendor processing PHI:
- Business Associate Agreement (BAA) with every vendor touching patient data
- Encryption in transit and at rest, consistent with NIST guidance
- Audit logging for all PHI-touching API calls
- Minimum-necessary data access controls
Compliance is the integration team's responsibility, not the vendor's alone.
What is FHIR and why does it matter for healthcare AI API integration?
FHIR is the current standard for structured healthcare data exchange, enabling AI applications to access patient records from EHR systems without custom data pipelines. SMART on FHIR extends this by allowing apps to launch inside EHR environments like Epic with patient context automatically populated at launch.
How long does healthcare AI API integration typically take?
Timelines range from weeks to six months or more, depending on complexity and the standards used. FHIR-based integrations using pre-built connectors are significantly faster than custom builds. Platforms like VectorCare's SoFaaS are designed to compress deployment from six months to a matter of weeks by providing pre-certified integration infrastructure.
What are the most common mistakes in healthcare AI API integration?
The top three: skipping sandbox testing and going directly to production, delegating HIPAA compliance entirely to the vendor rather than owning the full data flow, and scaling automation across multiple workflows before validating a single one. All three are avoidable with phased planning and explicit governance.
How do you measure the success of a healthcare AI API integration?
Define measurable KPIs before integration begins: reduction in manual coordination time, error rates, time-to-completion for key workflows, and staff hours saved per month. Without a documented baseline, ROI is impossible to demonstrate to leadership.