Introduction
An EHR integration strategy is the structured plan healthcare organizations use to connect electronic health record systems with clinical, operational, and logistics platforms — enabling real-time data exchange instead of manual workarounds.
For hospital IT leaders, transfer center managers, and health system administrators, this is no longer optional. A 2022 systematic review found that 7.9% to 18.1% of EHR-related patient safety events were attributed to interoperability failures. In one medication reconciliation study, 43.9% of current medications were missing from hospital records entirely.
ONC data shows 22% of hospitals still could not integrate received health information into their EHR without manual entry as recently as 2023.
Those numbers reflect a familiar pattern: most organizations respond reactively — building point-to-point connections to solve immediate problems, then inheriting a tangle of brittle interfaces that nobody fully understands.
This guide breaks down what a real EHR integration strategy looks like — and what separates the ones that hold from the ones that don't.
Key Takeaways
- EHR integration strategy is a structured plan governing how patient data flows automatically across connected systems, not a one-time IT deployment
- Fragmented data causes clinician errors, delayed discharges, redundant testing, and compliance risk
- Success requires FHIR-based standards, data governance from day one, a phased rollout, and cross-functional alignment
- SMART on FHIR enables logistics and care coordination tools to embed directly inside the EHR workflow
- Most integration failures trace back to governance gaps and poor change management — not technical problems
What Is an EHR Integration Strategy and Why Does It Matter?
EHR integration connects a health record system to other platforms — labs, billing systems, transport coordination tools, patient portals, home health agencies — so patient data moves automatically rather than being faxed, re-entered, or verbally communicated between staff.
Strategy means the deliberate plan governing which systems connect, in what order, using which standards, and toward what clinical or operational outcome. Without that plan, organizations end up with ad hoc, point-to-point connections built to fix immediate problems — creating technical debt that compounds over years.
The distinction between integration and interoperability matters here, because teams routinely conflate them:
- Integration = the technical connection that allows data to move between systems
- Interoperability = the receiving system can understand and act on that data meaningfully
You can have integration without interoperability. Data that arrives in the wrong format, mapped to the wrong fields, or stripped of clinical context is technically "integrated" but operationally useless.
Why This Matters for Frontline Operations
The consequences of poor integration aren't confined to the IT department. Consider what happens without it:
- Clinicians make decisions without complete medication histories
- Transfer coordinators spend 15–30 minutes per request making manual phone calls
- Discharge delays accumulate because transport requests can't be initiated from within the clinical workflow
- Billing teams rework claims when patient data doesn't match across systems
A 2022 systematic review found that interoperable smart-pump implementation reduced monthly data-entry keystrokes by 3.5 million across eight hospitals and cut manual programming errors by 19%.
That kind of result doesn't happen by accident — it's what a strategy makes possible. Defining target outcomes before implementation begins, rather than discovering failures after connections are built, is the difference between integration that transforms operations and integration that merely exists.
How EHR Integration Strategy Works: A Step-by-Step Framework
A well-executed integration strategy moves through five stages: assessment, architecture selection, data governance, phased execution, and continuous monitoring.
Step 1: Define Goals and Assess Current State
Integration strategy begins with a diagnostic. Before selecting any technology, organizations need to answer:
- Which systems currently exist, and which are disconnected?
- Where are clinical or operational decisions failing because of missing data?
- What regulatory requirements apply — HIPAA, the 21st Century Cures Act, TEFCA?
- Which specific use cases will integration address first?
That last question is critical. Integration must be driven by defined use cases — automating transport coordination, accelerating discharge planning, closing medication gaps at point of care — not by a vague goal to "connect systems." Without specific targets, projects drift: timelines slip, scope expands, and clinical staff end up with connected systems they don't trust or use.
Step 2: Choose the Right Architecture and Standards
The primary technical approaches available:
| Approach | Best For | Notes |
|---|---|---|
| FHIR R4 APIs | New integrations, patient access apps | ONC-mandated baseline since 2020 |
| HL7 v2 interfaces | Legacy system connections | Widely deployed, harder to maintain |
| Middleware/integration engines | Multi-system orchestration | Adds a normalization layer |
| SMART on FHIR | Third-party apps embedded in EHR | OAuth 2.0 authorization, context-aware launch |
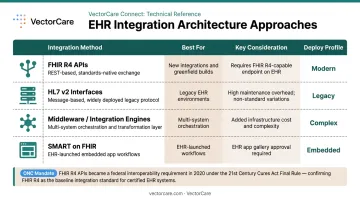
ONC's 21st Century Cures Act Final Rule adopted FHIR R4 as the standard for certified API technology, effective June 2020. By 2024, **81% of hospitals enabled app access through EHR APIs**, and 70% enabled FHIR-specific access — though adoption was higher among hospitals using market-leading EHR developers (83%) than others (56%).
SMART on FHIR deserves particular attention for logistics and care coordination use cases. It allows third-party applications to launch securely within the EHR environment, meaning transport coordinators, case managers, or transfer center staff can initiate workflows without leaving the clinical interface.
Two examples show what this looks like in practice. VectorCare's SMART on FHIR integration with Epic automatically pulls patient demographics and encounter data into transport requests, eliminating the manual re-entry that previously stretched single-transport coordination to 15–45 minutes. The Priority Dispatch Corp Medical Transfer Protocol (MTP) app — launched on the Epic Showroom through VectorCare's platform — embeds evidence-based interfacility transfer triage directly inside Epic, applying structured protocols the moment a transfer is initiated.
Step 3: Govern Data Before and During Integration
Data governance cannot wait until after integration is live. Organizations that skip this step encounter duplicate patient records, mismatched fields, and clinical staff who stop trusting integrated data.
Required from the start:
- Unified data model with standardized terminology (SNOMED CT, LOINC, ICD-10)
- Role-based access controls governing who can read, write, or modify integrated data
- Automated data quality checks before and after transfer
- PHI encrypted in transit and at rest, with full audit trail capabilities
- Business Associate Agreements in place with all connected vendors
Step 4: Execute in Phases
Phased implementation outperforms "big bang" approaches — better cost control, stronger stakeholder trust, and faster problem isolation.
A practical sequence:
- Phase 1: Select one or two high-impact use cases (lab result feeds, transport request automation). Validate thoroughly before expanding.
- Phase 2: Add adjacent workflows using lessons from Phase 1 (discharge planning integration, post-acute handoffs).
- Phase 3: Extend to additional facilities, payer connections, or new service lines as architecture matures.
When VectorCare processed its first 847 interfacility transfer requests in six weeks across four air operators and two hospital networks, the value of starting narrow and validating quickly was clear — each request represented coordination time that had previously been spent on sequential phone calls to multiple vendors.
Step 5: Monitor, Optimize, and Plan for Scale
Integration is not a one-time project. APIs update, regulations shift, and new facilities join health systems constantly. Organizations that treat integration as "done" typically find their connections break or fall out of compliance within 12–24 months.
Ongoing operational requirements:
- Performance monitoring: uptime, data latency, error rates, failed requests
- API version management as EHR vendors release updates
- A forward-looking roadmap for onboarding new systems or facilities
- Dedicated ownership — an integration capability requires a named owner, not occasional attention
Key Factors That Affect EHR Integration Strategy
Technical Standards and EHR Vendor Variability
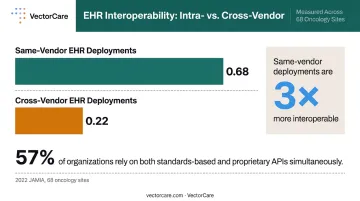
FHIR adoption does not equal plug-and-play integration. A 2024 JAMIA survey found that 85% of digital health companies supported FHIR, but only 61% used it extensively — and 57% relied on both standards-based and proprietary APIs simultaneously. Reported barriers included high API access fees (47%), lack of realistic testing data (41%), and limited data element access (40%).
Cross-vendor variability is even more pronounced. A 2022 JAMIA study across 68 oncology sites found mean intra-vendor interoperability of 0.68 versus cross-vendor interoperability of 0.22 — meaning same-EHR deployments are three times more interoperable than cross-vendor ones. Organizations integrating across Epic, Oracle Health/Cerner, and MEDITECH environments should budget explicitly for normalization logic.
Regulatory and Compliance Environment
Integration architecture is shaped by regulation, not just technology. Key compliance requirements:
- HIPAA: Technical safeguards required for all ePHI transmission
- 21st Century Cures Act: Information blocking violations can trigger penalties up to $1 million per violation for developers, HIEs, and HINs
- TEFCA: The nationwide health information exchange framework, with Qualified Health Information Networks designated starting December 2023
- State privacy laws: Vary by state, particularly for behavioral health and sensitive diagnoses
Compliance teams, legal counsel, and cybersecurity must be involved from the design stage — not consulted after architecture decisions are made.
Organizational Readiness and the Build vs. Buy Decision
Integration projects fail more often because of organizational issues than technical ones. Misaligned clinical workflows, absent executive sponsorship, and clinical staff who reject new tools because they disrupt established routines are the most common culprits. A 2025 scoping review found EHR-workflow misalignment was associated with communication challenges, documentation burden, and clinician task-switching at 1.4 times per minute.
Those organizational pressures make the build vs. buy decision even harder to get right. Custom integrations carry substantial implementation costs — proprietary API connections require significant effort for 52% of companies versus 40% for standards-based APIs. Ongoing maintenance tells a similar story:
| Integration Type | Significant Implementation Effort | Ongoing Maintenance Effort |
|---|---|---|
| Proprietary API | 52% of companies | 21% of companies |
| Standards-based API | 40% of companies | 13% of companies |
Pre-built platforms and SMART on FHIR as a Service (SoFaaS) models address this gap by enabling healthcare vendors to deploy EHR-embedded applications in weeks rather than months. VectorCare's forthcoming SoFaaS offering, for example, lets organizations skip rebuilding integration infrastructure for each new EHR environment — a meaningful reduction in both time and technical debt.
Common EHR Integration Challenges and How to Avoid Them
"Integration and Interoperability Are the Same Thing"
They are not. A technically successful data transmission that produces unusable clinical records is an integration success and an interoperability failure. Treating them as equivalent leads organizations to declare victory on connections that clinicians quietly stop relying on.
"FHIR Fixes Everything"
Teams that adopt FHIR and assume the normalization work is done typically discover within months that local data formats vary, EHR implementations differ significantly, and duplicate patient records have quietly accumulated. FHIR is a foundation, not a finished solution.
Treating Integration as a One-Time Project
EHR APIs update, regulations change, new facilities are added, and new use cases emerge. Organizations that integrate once and consider it complete frequently find connections break or become non-compliant within 12–24 months. Integration requires dedicated maintenance, monitoring, and a forward-looking roadmap — not just an initial deployment.
Ignoring Clinical Staff Adoption
Even technically sound integrations fail when clinical staff are left out of the design process. Common failure modes include:
- No clinical input during workflow design
- Insufficient training on new processes
- No clear explanation of how the integration affects daily practice
A documented example from VectorCare's platform illustrates the risk: a health system was experiencing a 12% SLA miss rate for dialysis transport pickups — not because the technical integration failed, but because clinicians were updating patient readiness status in Epic without a reliable mechanism to notify dispatchers.
The fix was rules-based automation that triggered a transport request automatically when readiness status changed. On-time performance climbed from 88% to 94% within one week. Automation handled what manual workflows couldn't do reliably: consistent, timely notification every time status changed.
Conclusion
Without a deliberate EHR integration strategy, organizations default to patchwork connections that drain IT resources, fragment data, and slow every team that depends on accurate patient information. Clinical, administrative, logistics, and care coordination platforms end up working in parallel rather than together.
The organizations performing best on patient outcomes and operational efficiency tend to have fewer silos, not fewer systems. A standards-based strategy built on FHIR, governed from day one, and executed in phases makes EHR data usable infrastructure — available to clinicians at the bedside, discharge planners coordinating post-acute care, and transport coordinators managing same-day logistics alike. Platforms like VectorCare's Connect module demonstrate what this looks like in practice: bi-directional EHR data exchange that removes manual handoffs from the patient logistics workflow entirely.
Frequently Asked Questions
What is an EHR integration?
EHR integration is the process of connecting an electronic health record system with other healthcare platforms — labs, billing systems, patient portals, or logistics tools — so patient data is exchanged automatically and securely without manual re-entry. Done well, it eliminates the manual handoffs that slow care delivery and create documentation gaps.
What is an example of an EHR integration strategy?
A hospital with discharge delays might implement a phased SMART on FHIR integration with Epic, automatically pushing patient data into transport coordination workflows to replace manual calls with documented handoffs. VectorCare's Epic integration works this way, pulling patient data directly into transport requests without staff leaving the clinical environment.
What are the five components of an EHR?
The core components of an EHR are patient demographics and history, clinical documentation, order management, results and reporting, and clinical decision support. Your integration strategy determines which of these components are accessible to external systems, and whether those systems have read-only or read-write permissions.
What are the four steps to a successful EHR implementation?
The four steps are: (1) assess current systems and define specific goals, (2) select the right architecture and standards for your environment, (3) execute in phases with thorough testing before expanding, and (4) train staff on new workflows and monitor performance continuously after launch.
What is the difference between EHR integration and interoperability?
Integration is the technical connection that allows data to move between systems: the pipe. Interoperability means the receiving system can actually understand and act on that data — what makes the water usable. You can have integration without interoperability if data arrives in formats the receiving system cannot process.
What role does FHIR play in EHR integration strategy?
FHIR (Fast Healthcare Interoperability Resources) is the current standard for healthcare data exchange, using RESTful APIs to share structured patient data across systems. SMART on FHIR extends this by letting third-party apps launch and operate inside the EHR environment, so staff complete workflows without switching platforms.