Introduction
Picture this: a patient is medically cleared for discharge at 10 a.m. The physician has signed the order. The care plan is complete. But at 2 p.m., that patient is still in their bed — because nobody has confirmed transport. A coordinator is on hold with the third ambulance company she's called this morning. Somewhere down the hall, an admitted ED patient is boarding because that bed isn't available yet.
This scenario plays out across U.S. hospitals every day. Clinical workflow optimization has traditionally focused on EHR documentation, scheduling efficiency, and care protocols inside the hospital.
That focus misses a critical truth: the care continuum — from admission through discharge to post-acute transition — is a single workflow problem. When any part of it breaks down, the cost shows up as longer stays, higher readmissions, and staff burnout.
This article covers:
- The most consequential bottlenecks slowing clinical workflows
- Strategies with measurable, documented results
- Why patient logistics coordination is the most underestimated piece of the puzzle
- How to measure whether optimization efforts are actually working
Key Takeaways
- Workflow optimization only reduces LOS and readmissions when applied across the full care continuum, not just within departments
- The highest-impact bottlenecks are often invisible — manual coordination, siloed systems, and fragmented care transitions
- Automating logistics tasks like transport dispatching can reclaim significant staff time without sacrificing clinical oversight
- EHR integration amplifies every other improvement — clinical data flowing into logistics workflows means faster action and fewer errors
- Track the right metrics — LOS, on-time performance, and coordination delays — to sustain gains past the initial rollout
What Is Clinical Workflow Optimization in Healthcare?
Clinical workflow optimization is the systematic redesign of how clinical tasks, information, and decisions move through a healthcare organization — with the goal of reducing waste, minimizing delays, and ensuring consistent, high-quality care delivery.
The scope is broader than most teams assume. Clinical workflows include:
- Patient admission and bed assignment
- Diagnostic testing and results routing
- Medication management and reconciliation
- Specialist consultations and handoffs
- Discharge planning and documentation
- Transport coordination and post-acute placement
All of these must work in concert. A breakdown in any one step delays every step that follows. Understanding where those breakdowns originate — and what type of fix each requires — is where workflow improvement actually begins.
Standardization vs. Automation
Two distinct mechanisms drive workflow improvement, and confusing them is a common mistake:
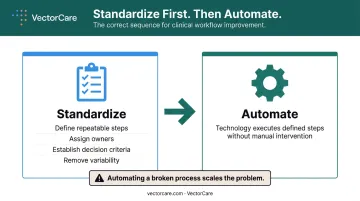
Workflow standardization defines repeatable processes with clear steps, owners, and decision criteria. It removes variability from how work gets done — before any technology touches it.
Workflow automation then uses technology to execute those defined steps without human intervention, freeing staff for work that requires clinical judgment.
Both are necessary, but order matters. Standardization without automation leaves staff executing well-defined processes by hand at scale. Automation without standardization simply accelerates broken ones. Standardize first, then automate.
Common Clinical Workflow Bottlenecks That Hurt Patient Outcomes
Siloed Systems and Documentation Burden
When clinical teams work across disconnected EHRs, scheduling tools, and communication platforms, they spend significant time manually reconciling information. A study of 155,000 U.S. physicians found average EHR time of 16 minutes and 14 seconds per encounter — with chart review, documentation, and ordering consuming 74% of that time combined.
That's time not spent on patients. At scale across an organization, the cumulative drag on clinical capacity is substantial.
Manual Communication: Phone, Fax, and the Coordination Tax
Despite decades of digital investment, analog communication persists across U.S. hospitals. In 2021, 78% of non-federal acute care hospitals still used mail or fax to receive summary-of-care records, according to ONC. The problem is structural, not a matter of preference.
When a discharge authorization, specialist consult, or transport request gets routed through a fax machine or a phone tag chain, every link in that chain is a potential delay point.
Discharge and Care Transition Delays
Discharge bottlenecks are among the most consequential workflow failures in a hospital. A UCLA study published in 2025 found that a standardized discharge pathway reduced median discharge-order-to-actual-departure time from 171 minutes to 88 minutes — cutting length of stay by 2.5 days for four common conditions.
Every occupied bed that belongs to a discharge-ready patient ripples outward: ED boarding increases, OR throughput drops, and system-wide capacity shrinks.
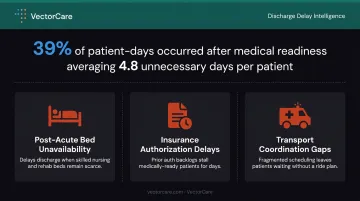
A neurology inpatient study found that 39% of patient-days occurred after medical readiness for discharge, averaging 4.8 medically unnecessary days per patient. The primary causes:
- Post-acute bed unavailability
- Insurance authorization delays
- Transport coordination gaps
Understaffing and Misaligned Staffing Models
Most clinical teams are scheduled based on historical patterns rather than real-time patient volume. A 2025 ED nursing study found that a deficit of just one nurse per hour below recommended staffing levels increased patient wait times by two minutes — with compounding effects as the gap widened.
The implication: even modest shortfalls carry measurable consequences. Demand-based scheduling closes this gap before it reaches patients.
Lack of Real-Time Visibility
When care coordinators, transfer centers, and clinical teams can't see where patients are in their care journey — or where delays are forming — they can't intervene early. This visibility gap is most acute during inter-facility transfers and post-acute transitions, where coordination happens across organizational boundaries with no shared tracking system.
Proven Strategies to Optimize Clinical Workflows
Standardize Before You Automate
Value-stream mapping is the right starting point for any high-volume care process — ED discharge, surgical prep, inter-facility transfer. The method requires mapping every step, distinguishing steps that add direct patient value from steps that represent waste, and redesigning the process before any technology is layered on top.
Standardized handoff protocols deserve specific attention. I-PASS implementation across nine academic hospitals was associated with a 23% relative reduction in medical errors and a 30% reduction in preventable adverse events. Structured communication templates for shift changes, specialist handoffs, discharge summaries, and transport requests reduce the variability that causes errors — independent of what technology is in use.
Integrate Systems to Enable Data Flow
The gap between EHR adoption and true interoperability remains significant. Hospital engagement across all four interoperability domains — sending, receiving, finding, and integrating patient data — rose from 46% in 2018 to 70% in 2023.
Yet in 2024, only 52% of clinical third-party integrations used standards-based APIs. For administrative workflows, that number drops to 35%.
Practical integration priorities:
- Connect EHR systems to operational tools (scheduling, transport coordination, post-acute placement) so patient data doesn't require manual re-entry at each handoff
- Configure EHR workflows to surface relevant information — pending orders, discharge criteria, patient history — at the right moment
- Require standards-based API connections for any new operational tool, not just EHR connectivity
Build a Culture of Continuous Improvement
Technology creates the capability; people and process determine whether it sticks. Nurses, transport coordinators, and discharge planners identify workflow friction weeks before it surfaces in LOS data — which is exactly why frontline staff should be active participants in redesign, not recipients of changes handed down by IT or management.
Establish regular review cadences with clear feedback loops. Effective metrics to track include:
- Length of stay — the most direct signal of coordination efficiency
- On-time transport and discharge performance — flags where handoffs break down
- Coordination delay rates — identifies recurring bottlenecks by shift or unit
Monthly or quarterly reviews tied to these metrics give teams the visibility to catch regressions early and sequence the next improvement cycle.
The Hidden Workflow Gap: Patient Logistics and Care Transitions
Intra-facility workflows have received most of the optimization attention over the past decade. The coordination of patient transport, inter-facility transfers, home health setup, and DME delivery has not.
This is the final mile of the clinical workflow — and it remains largely manual. The typical hospital transfer center or care coordinator is still:
- Calling transport providers one by one
- Waiting for callbacks while the patient waits in a bed
- Tracking status through phone notes or spreadsheets
- Managing availability windows with no real-time visibility
A Johns Hopkins analysis found that 30% of all patient-days involved a care delay, with lack of post-acute care beds accounting for 28% of those delays. Nobody measures discharge transport delays separately, which is precisely why the problem persists.
VectorCare was built on the recognition that patient logistics is an infrastructure problem, not a scheduling problem. The platform automates the logistics coordination layer that clinical workflow optimization has historically overlooked.
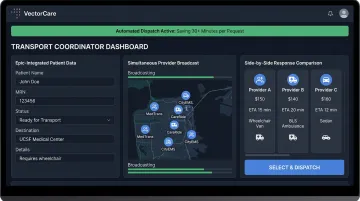
In practice, VectorCare's SMART on FHIR Epic integration transforms what was a 35-minute phone-based coordination process into approximately 90 seconds. Patient vitals and clinical data populate automatically from Epic. A single transport request then broadcasts simultaneously to multiple credentialed providers, with responses arriving in as little as 40 seconds and a side-by-side comparison presented to the coordinator in real time.
VectorCare's A.D.I. (Automated Dispatching Intelligence) takes this further by automating routine dispatching decisions entirely. Reported outcomes for hospital partners include a 45% reduction in communication-related delays, a 90% reduction in manual coordination tasks, and more than 100,000 staff hours saved across the platform by 2025.
When transport and post-acute coordination are automated and visible, care teams can plan discharges with confidence. Beds turn over faster. The next patient waiting in the ED gets placed sooner.
How Automation and Technology Drive Workflow Improvement
Automation earns its value by removing low-value, high-repetition tasks from clinical and administrative staff. The most common targets:
- Appointment reminders and scheduling confirmations
- Transport dispatching and logistics coordination
- Pre-registration data capture
- Insurance verification
McKinsey estimated that roughly 30 known interventions could deliver up to $265 billion in annual administrative savings across U.S. healthcare — most of which involves replacing manual processes with automated ones.
EHR Integration as a Foundation
Platforms that connect to EHR systems through standardized protocols like FHIR allow data to flow automatically into operational tools — reducing manual entry, ensuring accuracy, and enabling real-time coordination across departments. VectorCare's SMART on FHIR integration with Epic is a working example of this model: clinical data extracted from the EHR drives logistics decisions without burdening care coordinators with redundant data entry.
In 2022, 4 in 5 hospitals used APIs to enable clinician-facing apps to read from and write data to the EHR. The infrastructure exists. The gap is in extending that integration to operational and logistics workflows, not just clinical ones.
Automate the Right Things
That integration gap points to a broader caution: automation only improves outcomes when deployed on well-designed workflows. Automating a broken process produces broken outcomes faster.
The right sequence before selecting any technology:
- Assess the current state and map actual workflows
- Identify bottlenecks and failure points
- Standardize the process
- Implement technology on a workflow that's ready for it
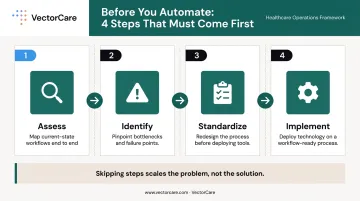
Skipping these steps doesn't accelerate improvement — it scales the problem.
Measuring and Sustaining Clinical Workflow Optimization
Metrics That Signal Whether Optimization Is Working
| Metric | What It Measures |
|---|---|
| Average length of stay | Overall care efficiency and throughput |
| Discharge-order-to-departure time | Execution quality of the discharge process |
| Avoidable days after medical readiness | Post-acute coordination and transport delays |
| Bed turnover rate | Capacity generation for incoming patients |
| On-time transport performance | Logistics coordination effectiveness |
| 30-day readmission rate | Care transition quality and follow-up |
| Staff time on administrative tasks | Automation and burden reduction impact |
AHRQ reported 13.9 readmissions per 100 index admissions in 2020, at an average cost of $16,300 per readmission. Adult readmissions cost Medicare $36.2 billion and Medicaid $11.4 billion that same year. Each of those dollars traces back to a care transition that broke down — a discharge delayed, a follow-up missed, a handoff that never happened.
Tracking these numbers identifies where breakdowns occur. Acting on them consistently requires the right organizational structure.
Governance That Sustains Gains
Workflow optimization is not a project. It is a continuous discipline. Organizations that treat it as a one-time initiative consistently see gains erode within 12–18 months as staff turnover, new processes, and shifting patient volumes create new gaps.
The organizational structures that sustain improvement include:
- A dedicated workflow improvement committee or operational excellence function
- Defined ownership for each key metric
- Established review cadences with authority to prioritize changes
- Clear escalation paths when performance regresses

Without this structure, improvements are one-off wins that fade. With it, the organization builds a repeatable process for identifying problems and acting on them before they compound.
Frequently Asked Questions
What is clinical workflow optimization in healthcare?
Clinical workflow optimization is the systematic improvement of how clinical tasks, information, and decisions flow across a healthcare organization. The goal is to reduce delays, eliminate waste, and ensure consistent, high-quality care delivery at every stage of a patient's visit.
How does clinical workflow optimization improve patient outcomes?
Streamlined workflows reduce diagnostic and treatment delays, improve coordination across care transitions, and free clinicians to focus on direct patient care. The result is shorter lengths of stay, fewer errors, and lower readmission rates — all measurable at the system level.
What are the most common bottlenecks in clinical workflows?
Siloed systems, manual communication via phone and fax, discharge and care transition delays, and lack of real-time visibility across departments are the most frequently cited sources of workflow friction. Post-acute placement delays and transport coordination add compounding delays that often go unmeasured.
Why is patient logistics considered part of clinical workflow?
Transport coordination, inter-facility transfers, and post-acute placement are the final mile of the clinical workflow. Delays in these steps directly extend length of stay, prevent beds from turning over, and increase downstream costs — making logistics coordination inseparable from clinical performance.
What role does automation play in clinical workflow improvement?
Automation handles routine, repetitive tasks — dispatching, reminders, data entry — freeing clinical and administrative staff for higher-value work. Its impact depends entirely on the quality of the underlying workflow: automating a broken process makes it fail faster.
How do hospitals measure the success of clinical workflow optimization efforts?
Key indicators include:
- Average length of stay and discharge-order-to-departure time
- Bed turnover rate and on-time transport performance
- Staff time on administrative tasks
- 30-day readmission rates
Sustained improvement requires tracking these within a governance structure that responds to regressions over time.