The real friction isn't in clinical care. It's in coordination: getting the right transport scheduled, confirming the discharge plan, closing the referral loop before a patient falls through it. That's where manual processes burn staff time, generate errors, and quietly widen care gaps.
This article examines three specific, measurable advantages of scheduling automation in healthcare — and what happens to operations, revenue, and patient outcomes when that automation is absent.
Key Takeaways
- Automated scheduling eliminates phone-heavy coordination across appointments, transport, referrals, and discharge
- Healthcare operations staff spend 20–30% of their day on nonproductive administrative tasks that automation can eliminate
- Automated reminders reduce missed appointments by roughly one-third, based on systematic review findings
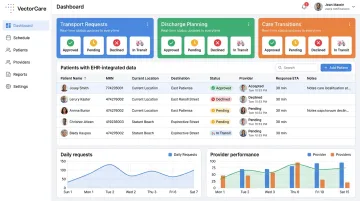
- EHR-integrated scheduling via SMART on FHIR eliminates manual data re-entry and gives coordinators real-time visibility across every care setting
- Automation compounds in value: consistent application across the patient journey drives down cost, delay, and error simultaneously
What Is Automated Patient Scheduling?
Automated patient scheduling uses software, AI, and intelligent workflows to manage booking, coordination, confirmation, and tracking of appointments and care transitions — without requiring manual effort at every step.
The scope spans the full care continuum:
- Enables self-scheduling, automated confirmations, and waitlist backfill for outpatient appointments
- Triggers transport scheduling directly from the EHR at the point of inpatient discharge
- Broadcasts NEMT requests to available providers and matches the right level of transport
- Converts fax-based referral intake into structured scheduling requests automatically
- Coordinates home health, DME delivery, and skilled nursing placement as a single discharge event
The more useful frame is infrastructure, not tooling. Scheduling automation determines whether patients receive care on time, beds turn over efficiently, and transport resources are matched correctly. Every phone call, manual handoff, and missed confirmation is a cost — and in high-volume systems, those costs compound fast.
Three Measurable Advantages of Scheduling Automation
Advantage 1: Elimination of Manual Coordination Overhead
Manual scheduling in healthcare is labor-intensive by design. A single patient care transition — discharge to home with transport, oxygen delivery, and a follow-up visit — can require a coordinator to make multiple phone calls, send faxes, re-enter data across disconnected systems, and wait for callbacks before a single event is confirmed.
McKinsey research on healthcare service operations found that staff typically spend 20% to 30% of daily work hours on nonproductive administrative tasks and idle time. This is a structural drag on capacity — one that compounds as patient volume grows.
The referral workflow is a clear example of where this breaks down. A JAMIA Open study on UCSF's referral automation tool found that 47% of incoming referrals arrived by fax, with manual entry averaging 719 seconds per referral — nearly 12 minutes of data entry per patient, before any scheduling actually happened. More striking: more than 40% of those referrals were never scheduled at all.
Automation addresses this directly:
- Intelligent dispatch systems broadcast requests simultaneously to available providers instead of calling them one at a time
- FHIR-integrated platforms auto-populate patient demographics, insurance, and clinical context from the EHR — eliminating re-entry
- Requests that previously took 35+ minutes to coordinate can be completed in under two minutes
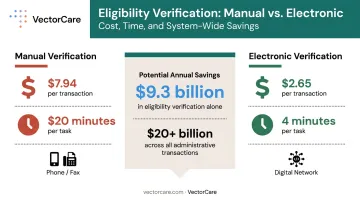
CAQH's 2023 Index reports that manual eligibility verification — a standard pre-scheduling step — costs $7.94 per transaction and takes 20 minutes. Electronic verification costs $2.65 and takes 4 minutes. Across millions of annual transactions, that gap represents $9.3 billion in potential annual savings on eligibility verification alone — with over $20 billion identified across all administrative transactions.
VectorCare's A.D.I. (Automated Dispatching Intelligence) platform puts a number on the operational impact. By 2025, A.D.I. had saved healthcare customers over 100,000 hours by eliminating manual coordination tasks across transport, discharge, and care transition workflows.
KPIs directly affected: staff hours per scheduled event, cost per coordination task, administrative labor cost as a percentage of operating expenses.
Advantage 2: Fewer No-Shows, Missed Transitions, and Care Delays
A missed appointment is a visible problem. A missed care transition — a patient discharged without confirmed transport, a home health visit that was never scheduled, a post-acute placement delayed because no one followed up — often isn't counted the same way, but the clinical and financial consequences are comparable.
No-show rates in outpatient settings typically range from 15% to 30%, with MGMA benchmarks showing median rates of 5–7% in better-performing practices. The missed-appointment problem is widespread enough that it shows up consistently in revenue, utilization, and readmission data.
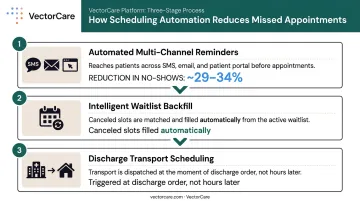
Automated reminder systems reduce that gap meaningfully. A 2016 systematic review synthesizing 11 systematic reviews and 31 randomized controlled trials found a weighted mean relative reduction in non-attendance of 34% from baseline across reminder interventions — with automated reminders contributing roughly a 29% relative reduction. The finding holds across diverse care settings, making it a reliable benchmark for planning.
For NEMT-dependent patients, the stakes are higher. Research shows transportation barriers cause 3.6 million people to delay or miss care annually, and transportation interventions are associated with a pooled odds ratio of 0.63 for missed clinic visits — meaning patients with coordinated transport attend at materially higher rates.
Scheduling automation targets the problem at each stage of the appointment lifecycle:
- Automated multi-channel reminders (SMS, email, patient portal) reduce no-shows before they happen
- Intelligent waitlist backfill fills canceled slots automatically, recovering revenue from appointment slots that would otherwise go unused
- Discharge transport scheduling triggered at the time of the discharge order — rather than hours later — reduces the coordination delays that hold patients in beds past clinical readiness
The bed-day cost of coordination failure is real. KFF reports average US hospital expenses of $3,297 per adjusted inpatient day in 2024. Every day a patient remains in an acute bed because post-acute placement or transport wasn't confirmed in time is a direct cost to the system — compounded across thousands of discharges annually.
UCSF's EHR-based automated self-rescheduling tool demonstrates the revenue recovery angle: it filled 6,703 appointment slots in 9 months, added 2,576 patient service hours, and generated an estimated $3 million in professional fees from slots that would likely have remained empty.
KPIs directly affected: no-show and cancellation rate, appointment slot utilization, average length of stay, 30-day readmission rate.
Advantage 3: Real-Time Visibility and EHR-Integrated Coordination
One of the most persistent scheduling problems in healthcare is fragmentation, not volume. Patient data lives in the EHR. Transport requests go through a separate system. Home health coordination happens by phone.
No single view exists of where a patient is in their care journey — so coordinators spend their time reacting to information gaps rather than managing proactively.
Modern scheduling automation resolves this through direct EHR integration using standards like SMART on FHIR. When a coordinator initiates a transport or discharge request from within Epic, FHIR APIs automatically extract:
- Patient demographics and insurance
- Scheduled procedures and appointment times
- Clinical context (acuity, equipment needs, fall risk)
- Current location and discharge destination
Nothing is re-entered. Every logistics event — transport, DME, home health referral — is pre-populated with verified data from the patient's existing chart.
EHR adoption in US acute care hospitals reached 99.4% in 2024 (ONC), and approximately 9 in 10 hospitals now enable patient data access via apps through FHIR-compliant APIs. The infrastructure for integrated scheduling already exists in most health systems — the gap is in connecting logistics workflows to it.
VectorCare's Connect module integrates with Epic, Cerner/Oracle Health, Meditech, Athenahealth, and any FHIR-compliant EHR. When the integration is active, the full transfer coordination process compresses from a 35-minute phone-based workflow to approximately 90 seconds.
Providers respond to simultaneously broadcast requests in as little as 40 seconds. Status updates and arrival confirmations write back to the EHR automatically — no manual documentation required.
The clinical downstream benefit is concrete. When transport, discharge, home health, and DME scheduling are visible in one place, care teams act on real information rather than chasing confirmations. Coordination gaps that generate readmissions, extended stays, and patient safety risk become visible before they become problems.
VectorCare's platform has documented a 45% decrease in communication-related delays across its customer base — a direct result of coordinators having unified visibility rather than hunting across disconnected systems.
KPIs directly affected: scheduling data accuracy, communication-related delay rate, time from discharge order to patient departure, on-time transport performance, EHR documentation completeness.
What Happens When Scheduling Automation Is Missing
Manual scheduling doesn't fail catastrophically — it fails incrementally, and the costs get normalized.
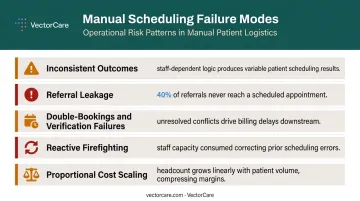
Common failure modes in manual scheduling environments include:
- Inconsistent outcomes driven by individual staff knowledge rather than standardized logic — two coordinators handle the same scenario differently, and neither outcome is tracked
- Referral leakage — in a large health system study, low documented scheduling rates in the EMR accounted for 40% of the gap in closing the referral loop
- Double-bookings and insurance verification failures that generate billing delays well after the patient has been seen
- Reactive firefighting — staff spend time correcting yesterday's scheduling errors instead of managing today's care proactively
- Proportional cost scaling — as patient volume grows, manual coordination headcount must grow with it, because nothing about the process gets more efficient
The administrative burden also drives burnout. The National Academy of Medicine identifies reducing documentation and administrative burden as a national health workforce priority, and JAMA Health Forum links clerical task volume directly to clinician well-being and retention.
That staff-side pressure has a direct patient-side consequence. For logistics-dependent populations — including Medicaid patients, chronic condition patients, and those relying on NEMT — unreliable scheduling narrows care access in ways that compound over time. Missed transport means missed care, with clinical consequences that surface later as readmissions or emergency visits.
How to Get the Most Value from Scheduling Automation
Partial automation leaves most of the value on the table. Automated reminders without integrated dispatch, or automated dispatch without EHR integration, create new handoff gaps rather than closing existing ones.
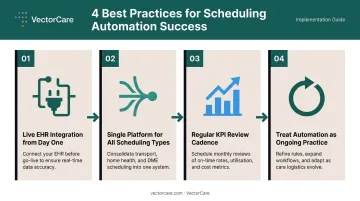
Scheduling automation performs best when:
- EHR integration is live from day one — data flows automatically and coordinators stop managing parallel processes
- All scheduling types run through a single platform — transport, home health, DME, and discharge logistics coordinated together, not solved in isolation. VectorCare is purpose-built for this across 2,500+ healthcare facilities
- KPIs are reviewed on a regular cadence — no-show rates, coordination time, on-time transport performance, and LOS metrics tracked against automation benchmarks, not measured once at go-live
- Automation is treated as ongoing practice — configuration, monitoring, and incremental refinement deliver measurably better outcomes over time as the system learns usage patterns and staff build confidence in automated workflows
The economics support sustained investment. A California hospital system documented $22 million in annual savings after implementing VectorCare Hub to coordinate discharge-related logistics — transport, medical equipment, home oxygen, and post-discharge services — within a unified platform. Those savings came from reducing delays, shortening length of stay, and eliminating the manual coordination overhead that piecemeal tools leave behind.
Conclusion
Scheduling automation in healthcare is an infrastructure decision — one that determines whether care coordination holds together under volume pressure or breaks down at the seams. Organizations that treat it as a back-office function will keep absorbing the costs that manual coordination quietly accumulates: missed appointments, delayed discharges, staff hours lost to phone calls.
Eliminating manual overhead, reducing missed appointments and care transition gaps, and gaining real-time EHR-integrated visibility each address a distinct failure point. Combined, they shift the operational baseline — less rework, fewer delays, and coordination that doesn't depend on any one person remembering to make a call.
Organizations that invest in scheduling infrastructure can grow patient volume without adding administrative headcount, improve throughput without adding beds, and free clinical staff from the coordination overhead that drives burnout. That's not an incremental improvement — it's a structural change in how care gets delivered.
Frequently Asked Questions
What is automated patient scheduling in healthcare?
Automated patient scheduling uses intelligent software and AI to handle booking, dispatch, reminders, and care coordination without requiring manual intervention at each step. That spans outpatient appointments, NEMT coordination, discharge planning, and post-acute transitions — all managed through a single integrated workflow.
How does scheduling automation reduce hospital length of stay?
Automation reduces LOS by eliminating the coordination delays that keep patients in beds past clinical readiness. When transport, post-acute placement, and home health scheduling are automated and integrated with the EHR, discharge workflows execute faster and with fewer gaps between steps.
What are the most common scheduling challenges that automation solves?
The most common pain points automation addresses include:
- Manual phone-based coordination across care teams
- High no-show and missed-transition rates
- Referral leakage, where 40%+ of referrals are never scheduled
- Double-bookings and insurance verification delays
- No real-time visibility into patient scheduling status across care settings
How does scheduling automation integrate with EHR systems?
Modern platforms use standards like SMART on FHIR to embed directly into EHR environments, automatically pulling patient demographics, insurance, and clinical data into scheduling workflows without manual entry. Coordinators initiate and manage logistics without leaving their existing clinical tools.
Is automated patient scheduling secure and HIPAA-compliant?
Enterprise-grade scheduling platforms operate on HIPAA-secure cloud infrastructure with role-based access controls, structured data transmission protocols, and centralized audit trails that replace the compliance risks inherent in phone calls and fax-based exchanges.
When does scheduling automation deliver the highest ROI?
ROI is highest in high-volume, high-complexity environments: transfer centers, health systems managing daily discharge transitions, and NEMT-dependent patient populations. These are the settings where the time and error cost of manual coordination is greatest and most directly measurable.