According to the AONL's 2025 Nursing Leadership Insight Study, only 27% of nurse leaders identified flexible scheduling as one of the most helpful tools for improving staff morale — meaning most facilities aren't yet using scheduling strategically as a retention and quality lever.
Most health systems still treat scheduling as a back-office administrative function. That's the core problem. A growing number are turning to outside expertise to correct it — not because they lack calendars, but because they lack the analytical frameworks to align staffing patterns with actual operational demand.
This article covers what healthcare staff scheduling consultants actually do, where they drive the most impact, how to recognize when you need one, and what separates a credible consultant from a generic management firm.
Key Takeaways
- Scheduling consultants audit, redesign, and implement staffing frameworks — they don't just optimize shift fills
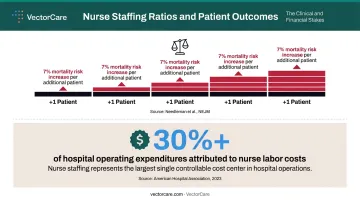
- Nurse labor accounts for over 30% of hospital expenditures, making scheduling accuracy a financial imperative
- Each additional patient per nurse is associated with a 7% increase in 30-day mortality risk
- Delayed discharges cost an average of $39,103 per patient, with transport coordination failures a leading driver
- Technology and consulting work together; neither substitutes for the other
What Does a Healthcare Staff Scheduling Consultant Do?
A healthcare staff scheduling consultant is an external expert who assesses a facility's existing scheduling ecosystem, identifies inefficiencies, and redesigns processes to align staffing with operational demand and patient care needs. The role is diagnostic before it is prescriptive.
The Assessment Phase
Consultants begin with a deep audit — reviewing current schedules, staffing models, shift rotations, and historical data to identify patterns. They're looking for:
- Chronic understaffing or overstaffing by unit and shift
- Excess overtime driven by last-minute coverage gaps
- Agency and traveler reliance that signals systemic scheduling dysfunction
- Shift inequities that create staff grievances
The goal is to surface the structural patterns causing recurring problems — not assign fault.
Design and Implementation
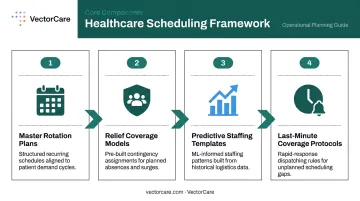
After diagnosis, consultants build customized scheduling frameworks. These typically include:
- Master rotation plans matched to patient volume patterns
- Relief coverage models that reduce agency dependency
- Predictive staffing templates that account for seasonal demand and specialty mix
- Protocols for handling last-minute coverage without defaulting to overtime
The framework is built around the facility's specific size, service lines, union agreements, and regulatory environment — not adapted from a generic template.
Analytics, Technology, and Ongoing Advisory
Once a framework is in place, workforce analytics tools take over the ongoing work of anticipating demand. Consultants use historical data and volume patterns to build schedules that get ahead of peak care periods rather than scrambling to respond to them.
Many engagements extend beyond initial implementation. Consultants train operational leaders to maintain and evolve the scheduling model over time, with the explicit goal of building internal capability so the facility isn't reliant on outside support indefinitely.
Key Areas Where Scheduling Consultants Drive the Most Impact
Nurse and Clinical Staff Scheduling
Nurse labor costs account for over 30% of all hospital expenditures, making it the highest-stakes scheduling domain in most acute care settings. When that labor isn't deployed efficiently — when overtime substitutes for proper planning, or agency staff fill gaps that shouldn't exist — the financial exposure compounds quickly.
Nurse scheduling is also the most legally and operationally complex domain:
- Seniority and union rules govern shift assignment in many systems
- Mandatory rest periods vary by state and contract
- Licensure requirements limit who can cover what
- Equitable distribution of nights, weekends, and holidays affects retention as much as pay
Consultants who specialize in nurse scheduling understand these constraints as a system. They don't just fill shifts — they design rotation models that distribute burden fairly while meeting coverage requirements across all units.
The safety stakes matter here. AHRQ data shows each additional patient assigned per nurse is associated with a 7% increase in 30-day mortality odds. Those numbers make nurse scheduling one of the few operational decisions with a direct line to patient outcomes.
Patient Transport and Discharge Logistics
Patient transport and discharge coordination are where scheduling consultants often uncover the most overlooked inefficiencies. Delayed discharges are expensive: a systematic review found the average cost per delayed patient reaches $39,103, with excess bed-days accounting for up to 30.7% of total costs in some cases.
The underlying cause is rarely a transport shortage. More often, it's a coordination workflow failure: handoffs between clinical staff, transport providers, home health agencies, and DME suppliers that don't sync. Consultants examine these handoff points specifically — where scheduling misalignment between teams extends hospital stays that could end hours earlier.
VectorCare's platform, which serves over 2,500 healthcare facilities, addresses this at the infrastructure level — embedding patient logistics coordination into EHR workflows and automating dispatch through its ADI (Automated Dispatching Intelligence) technology to eliminate the manual handoffs that create delays.
The results are concrete. Facilities using the platform have reduced the oxygen discharge ordering process to 3–5 minutes, replacing a phone-based workflow that previously kept patients inpatient for an extra one to two days. What looks like a scheduling gap is often an infrastructure gap — and closing it requires both operational expertise and the right tooling.
Signs Your Facility Needs a Healthcare Scheduling Consultant
Some signals are obvious. Others take longer to surface.
Clear operational warning signs:
- Transport and coordination costs that consistently outpace budget with no seasonal explanation
- Heavy reliance on contracted or third-party vendors to fill routine logistics gaps
- Care team complaints about coordination failures and unpredictable transport turnaround times
- Recurring shift coverage failures that compromise patient-to-staff ratios
Subtler signals that often go unrecognized:
These are harder to catch because they rarely show up as line items — they surface as pattern anomalies buried in operational data:
- Discharge delays attributed to "transport availability" when the root cause is coordination workflow
- EHR data showing discharge times clustering in late afternoon rather than mid-morning
- McKinsey reported that 31% of nurses still intended to leave their jobs in 2023 — scheduling unpredictability and logistics friction are consistently cited among the drivers
- Repeat readmissions or post-discharge gaps that trace back to handoff breakdowns rather than clinical decisions
Facilities undergoing growth, expanding into new service lines, or navigating system mergers are especially vulnerable. Each new layer of complexity accelerates the dysfunction already present — and by the time it shows up in financial reports, the operational damage is months old. Catching these signals early is what separates a targeted workflow fix from a full-scale crisis response.
The Real ROI: What Facilities Gain from Scheduling Expertise
Cost Reduction
The AHA reported hospitals were paying $24 billion more per year for clinical labor during the pandemic period, with clinical labor costs rising an average of 8% per patient day — driven largely by agency and temporary labor use. That's the cost of reactive staffing.
Proactive scheduling redesign directly attacks that spend. A 2024 rapid review of centralized nursing staff scheduling found consistent patterns: less overtime, less contracted labor, and more balanced staffing across facilities that made the shift.
Mercy Health's internal gig workforce initiative — documented in AHA's 2024 Workforce Scan — reduced agency spend by $5 million while achieving an 86% fill rate using internal staff. Jefferson Health's SEAL team model met 12–16% of weekly staffing needs through self-scheduling, saving millions annually. These results come from redesigned scheduling systems, not technology alone.

Staff Retention
NSI's 2026 report puts the average cost of bedside RN turnover at $60,090 per nurse, with average annual hospital RN turnover costing $5.19 million. Every 1% change in RN turnover rate corresponds to approximately $294,976 in cost or savings.
Scheduling instability is one of the most frequently cited contributors to nurse attrition. Consultants who redesign schedules to improve fairness, predictability, and work-life balance address one of the most actionable levers for retention — without requiring compensation changes.
Quality of Care
A 2021 peer-reviewed study confirmed that nurse staffing levels are directly associated with missed care, which in turn correlates with adverse patient outcomes. When scheduling produces chronic understaffing — even intermittently — care quality suffers in measurable ways.
Compliance and Risk
In heavily regulated states, scheduling errors carry direct financial penalties:
- California (CDPH): $15,000 for a first staffing ratio violation; $30,000 for subsequent violations
- Oregon (HB 2697): Enforceable staffing requirements with civil penalties attached
- New York (Labor Law §167): Restrictions on mandatory overtime for nurses
Non-compliance isn't just an operational risk — it's a balance sheet risk that grows with every unmanaged gap.
What to Look for in a Healthcare Scheduling Consultant
Experience That Matches Your Context
Generic operations consultants and healthcare scheduling specialists are not interchangeable. Domain-specific experience matters: facility type (acute care, skilled nursing, NEMT operations), applicable union agreements, state labor regulations, and a track record of measurable outcomes.
Consultants like VectorCare's Craig Ruggels — with 15+ years working across Kaiser Permanente, Sutter Health, and Dignity Health — bring operational knowledge no generalist can replicate. That firsthand familiarity with California's most complex health systems enables precise diagnosis, not just generic recommendations.
Methodology Indicators
A consultant worth hiring has a structured process. Look for:
- A defined assessment phase with data review before any recommendations
- Data-driven recommendations — not intuition-based
- A phased implementation plan that accounts for staff change management
- A training component that transfers capability to internal leaders
Avoid engagements that produce a report and disappear — the real value is in implementation and knowledge transfer.
Credentials vs. Experience
Degrees in healthcare administration, industrial-organizational psychology, or operations management are common among experienced consultants. They're useful context. Practical experience with real scheduling systems, real union agreements, and real regulatory environments carries more weight in hiring decisions. When evaluating candidates, let the operational track record drive the decision.
How Technology Amplifies a Consultant's Recommendations
The best scheduling framework underperforms without the right infrastructure to support it. Consultants today evaluate and often recommend scheduling platforms and workflow automation tools as part of their deliverables.
Modern platforms do several things that manual coordination cannot:
- Automate dispatching and reduce per-coordination task time dramatically
- Provide real-time visibility into resource availability across the system
- Generate the analytics data consultants need to diagnose problems and measure improvements
- Integrate with EHR systems to create bidirectional data flows that eliminate manual entry
VectorCare's platform reduces transport scheduling from an average of 31 minutes per coordination call to under two minutes in air transport scenarios, dropping to as little as 47 seconds in some EHR-embedded workflows. For facilities where discharge coordination bottlenecks are extending length of stay, that's a direct impact on bed availability and throughput.
The consultant-technology relationship runs both ways. The best consultants are tool-agnostic — they help facilities select or configure platforms that match specific workflow needs, not just the ones a vendor happens to sell. A consultant who prescribes one solution regardless of context is worth questioning.
Frequently Asked Questions
What does a healthcare scheduling consultant do?
A healthcare scheduling consultant assesses, redesigns, and optimizes a facility's staffing and scheduling processes to improve patient care, reduce costs, and increase staff satisfaction. Engagements typically cover everything from master rotation design and agency dependency reduction to analytics implementation and leader training.
How much does a healthcare scheduling consultant charge?
Fees vary widely by scope, facility size, and engagement model. Project-based fees for initial assessments, retainer arrangements for ongoing advisory, and day rates for specialized engagements are all typical structures. No standard public rate card exists for this specialty; most firms provide custom proposals based on facility complexity and engagement requirements.
Do you need a degree to be a healthcare scheduling consultant?
Degrees in healthcare administration or operations management are common entry points, but most facilities prioritize demonstrated operational experience, a proven methodology, and knowledge of applicable labor regulations over academic credentials alone.
How long does a healthcare scheduling consulting engagement typically last?
Initial assessment and redesign engagements commonly run 3–6 months. Ongoing advisory relationships can extend longer depending on facility complexity, the extent of changes required, and whether staff training and change management are part of the engagement.
How do I know if my facility needs a healthcare scheduling consultant?
Persistent overtime budget overruns, heavy reliance on agency staff, high clinical staff turnover, or chronic patient throughput delays that trace back to coverage and coordination gaps are the most actionable signals. If any of these have persisted for more than two consecutive quarters, a consultant assessment will typically cost far less than another quarter of compounding overtime and agency spend.
What is the difference between a scheduling consultant and scheduling software?
Software automates and executes scheduling tasks. A consultant diagnoses systemic problems, redesigns workflows, and guides the people and processes around the technology. The two work best together: software without the right workflow design underperforms, and workflow redesigns without supporting technology don't scale.