Introduction
Most hospitals run on a patchwork of disconnected software — EHRs, scheduling platforms, billing systems, transport coordinators — and the gaps between them cost clinical staff hours every week. When patient data doesn't move automatically between systems, someone has to move it manually: phone calls, fax machines, re-entered demographics, and reconciled records that should never have diverged in the first place.
EHR API integration addresses this directly. The operational payoff is concrete: faster care transitions, fewer documentation errors, less administrative burden on nurses and coordinators, and better-coordinated patient logistics across every handoff point.
This article breaks down what EHR API integration actually is, the key standards driving it, and the measurable operational advantages healthcare organizations see when they get it right.
Key Takeaways
- EHR API integration connects disparate healthcare platforms so patient data flows automatically, eliminating manual re-entry and information silos
- The leading standards — FHIR R4, HL7 v2, SMART on FHIR, and USCDI — each serve a distinct role in the interoperability stack
- Key advantages include real-time clinical data access, improved care coordination across settings, and a clearer path to regulatory compliance
- Information blocking violations carry civil monetary penalties up to $1 million per violation for health IT developers and health information networks
- Integration delivers compounding returns when treated as ongoing infrastructure rather than a one-time technical project
What Is EHR API Integration?
EHR API integration is the process of using Application Programming Interfaces (APIs) to allow an EHR system to securely share and receive patient data with other healthcare software platforms — labs, scheduling tools, patient portals, transport coordination systems, billing platforms — in real time and without manual intervention.
It applies across hospitals, health systems, skilled nursing facilities, transfer centers, payers, and any organization where patient data needs to move between multiple clinical or operational platforms.
What it enables matters more than how it works: faster clinical decision-making, fewer data errors, less staff burden, and better continuity of care across the full patient journey.
Key EHR API Integration Standards
Four standards define the current interoperability landscape:
FHIR R4: The primary API specification mandated under the ONC Interoperability Rule via the 21st Century Cures Act. Uses RESTful architecture and JSON formatting, requiring certified health IT developers to expose patient data through standardized API endpoints. Verify the compliance deadline applicable to your organization type.
HL7 v2: The legacy messaging standard still running in most hospital systems for orders, admissions, and lab results. Pipe-delimited and not web-native, but deeply embedded in existing infrastructure. According to the National Library of Medicine, HL7 v2 remains the most widely used health information exchange standard in the US — necessary for older platforms, but not a long-term path to interoperability compliance.
SMART on FHIR: The OAuth 2.0-based authorization framework that controls how third-party applications securely access EHR data with scoped permissions. It's the standard mechanism for launching external tools — patient logistics platforms, care coordination apps, prior authorization systems — directly within an EHR environment.
USCDI (United States Core Data for Interoperability): The federal specification defining the minimum patient data elements certified EHRs must expose through their APIs — demographics, problems, medications, allergies, labs, and care plans. ONC published USCDI v6 in July 2025, with v7 in draft as of early 2026.
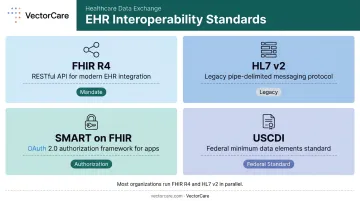
These standards coexist rather than replace each other. Most organizations run FHIR R4 for modern integrations while maintaining HL7 v2 connections for legacy systems in parallel.
Key Advantages of EHR API Integration
The advantages below focus on measurable, operational impact — outcomes that hospital administrators, clinical leaders, and operations teams track: cost, efficiency, error rates, care quality, and compliance risk.
Real-Time Patient Data Access
EHR API integration gives every connected platform instant access to current patient data (diagnoses, medications, allergies, vital signs, care plans) without staff manually pulling or re-entering information between systems.
In practice: rather than a coordinator calling to confirm patient status or re-entering demographic data into a transport platform, the API pulls that data automatically at the moment it's needed. Research shows physicians spend a median of 36.2 minutes on EHR tasks per visit — a significant portion of which involves data retrieval and reconciliation that integrated systems eliminate.
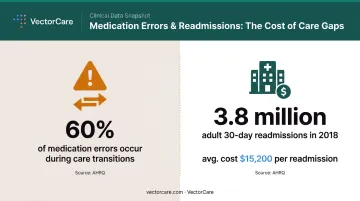
The patient safety implications are direct. AHRQ estimates that 60% of medication errors occur during transitions of care — precisely the moments when incomplete or delayed records create the most risk. When a transport coordinator or transfer center has real-time access to a patient's current condition, transport mode decisions happen faster and more accurately.
KPIs this advantage influences:
- Time-to-decision for care transitions
- Data entry hours per staff member per week
- Documentation error rates
- Time from EHR order to transport dispatch
High-volume settings feel this most acutely. In transfer centers, emergency departments, and patient logistics hubs processing dozens of transitions daily, each retrieval delay compounds across the entire census.
Improved Care Coordination Across Settings
EHR API integration allows every stakeholder in a patient's care journey (primary care, specialist, hospital, transport provider, home health agency) to work from the same current clinical picture rather than fragmented or delayed records.
When a patient is discharged and a transport request is initiated, an EHR-integrated platform can automatically pull the patient's current diagnosis, mobility needs, and destination details from the EHR rather than requiring a nurse to manually complete a referral form. This is the model VectorCare's SMART on FHIR Epic integration uses — automatically extracting patient demographics, encounter details, vitals, and clinical context from Epic to trigger and route transport requests without manual coordination steps.
The transaction is documented back in the medical record, closing the loop within the clinical workflow.
Care coordination failures most often occur at transitions (discharge, transfer, handoff) where incomplete or delayed patient information forces the receiving team to act without full clinical context.
A structured handoff intervention published in the New England Journal of Medicine reduced medical errors from 24.5 to 18.8 per 100 admissions and preventable adverse events from 4.7 to 3.3 per 100 admissions — illustrating how better information handoff directly translates to better outcomes.
AHRQ reported 3.8 million adult 30-day all-cause readmissions in 2018 at an average cost of $15,200 each. Not all readmissions trace back to coordination gaps — but research consistently links health information exchange with reduced duplicate testing and lower system-level costs.
KPIs this advantage influences:
- Length of stay
- Hospital readmission rates
- Time from discharge order to transport dispatch
- Manual calls or faxes per transfer
- Duplicate test rate
This advantage is most critical in multi-facility health systems, transfer centers managing high volumes of inter-facility moves, and patient logistics platforms coordinating across ambulance providers, home health agencies, and SNFs simultaneously.
Regulatory Compliance and Standards Readiness
EHR API integration built on FHIR and USCDI standards positions organizations to meet current and upcoming federal interoperability mandates — rather than scrambling to retrofit compliance later.
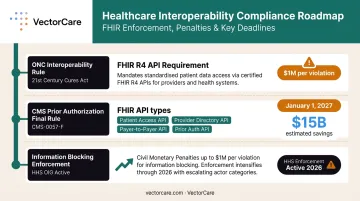
The compliance landscape has three key components:
- ONC Interoperability Rule / 21st Century Cures Act — Requires certified health IT developers to expose FHIR R4 APIs for patient data access. Information blocking violations can carry civil monetary penalties up to $1 million per violation for health IT developers and health information networks/exchanges.
- CMS Prior Authorization Final Rule (CMS-0057-F) — Requires affected payers (Medicare Advantage, Medicaid, CHIP, and QHP issuers on federally facilitated Exchanges) to implement FHIR-based Patient Access, Provider Access, Payer-to-Payer, and Prior Authorization APIs. API compliance dates generally begin January 1, 2027. CMS estimates the rule will generate approximately $15 billion in savings over 10 years.
- Information Blocking Enforcement — HHS enforcement activity has entered a new phase in 2026, making this no longer a theoretical risk.
Organizations with mature FHIR API infrastructure can connect to more partner platforms, qualify for value-based care arrangements requiring data sharing, and avoid the technical debt of retrofitting legacy systems to meet new mandates.
KPIs this advantage influences:
- Information blocking incident rate
- Prior authorization processing time
- Cost of compliance remediation
- Number of partner platforms supported through standardized API endpoints
This advantage carries the highest urgency for hospitals in value-based care arrangements, payers subject to CMS Prior Authorization deadlines, and any organization currently using proprietary or point-to-point integrations that won't scale to future standards.
What Happens When EHR API Integration Is Missing
The consequences aren't abstract — they show up in daily operations.
Four operational gaps surface immediately when integration is absent:
- Staff time lost to manual data work: Clinical teams spend hours each week re-entering, reconciling, or tracking down patient data across disconnected systems. MGMA reports that in 2023, 89% of practices said prior authorization was very or extremely burdensome, with 92% hiring or redistributing staff just to manage PA volume.
- Care decisions made on incomplete data: Without real-time data sharing, care transitions rely on fragmented information. The wrong transport mode gets dispatched. The receiving facility isn't prepared. Medications get re-ordered because prior results aren't visible.
- Compliance exposure that compounds over time: As federal mandates tighten, organizations on legacy HL7 v2 interfaces face growing information blocking risk and expensive remediation timelines. Retrofitting non-compliant systems costs more than proactive integration.
- Growth that requires more headcount, not smarter workflows: Manual coordination doesn't scale. Without EHR API integration, adding patient volume means adding staff to do the same work — not automating it.
How to Get the Most Value from EHR API Integration
EHR API integration delivers compounding returns when applied consistently across the full patient care workflow — not just at one point of care.
Prioritize high-impact integration points first:
- Discharge and transfer workflows
- Lab result delivery
- Prior authorization
- Transport coordination triggers
Measure outcome improvement at each step, then expand from there. An all-at-once enterprise rollout rarely succeeds.
Plan for ongoing maintenance, not a one-time deployment. EHR vendors release API updates that can break existing connections. Staying current requires attention to:
- USCDI data element changes (v6 is current; v7 is already in draft)
- OAuth token management and refresh cycles
- Health system-specific configuration updates
Organizations that treat EHR API integration as a finished project see performance degrade within 12–18 months without active maintenance.
Purpose-built platforms cut the build time significantly. For organizations embedding EHR API capabilities into patient logistics workflows, VectorCare's SoFaaS (SMART on FHIR as a Service) removes the need to build from scratch. SoFaaS enables healthcare vendors and logistics platforms to build, deploy, and scale EHR-embedded applications in weeks rather than months, beginning with Epic, without requiring dedicated health IT engineering teams.
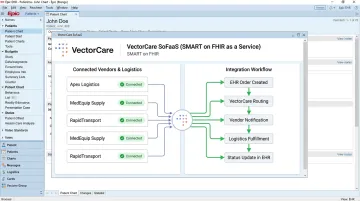
The platform handles SMART on FHIR compliance, security governance, HIPAA requirements, and health system installation — so partners can focus on care delivery rather than integration infrastructure.
Conclusion
EHR API integration earns its place in health system infrastructure because of what actually changes downstream: clinicians act on complete information, care transitions don't stall at handoffs, and compliance teams stop chasing documentation retroactively.
The advantages compound over time when integration is treated as ongoing infrastructure. Real-time data access, coordinated care across settings, and regulatory future-proofing each reinforce the others — and each degrades without active maintenance.
As interoperability mandates continue expanding and patient care increasingly spans multiple settings and providers, organizations that build on standards-based EHR API integration now are positioned to absorb that complexity without adding staff or manual workarounds. For health systems coordinating transport, post-acute care, and ancillary services — areas where VectorCare's SMART on FHIR integration operates — that infrastructure difference shows up directly in discharge timelines, bed utilization, and readmission rates.
Frequently Asked Questions
What is the difference between FHIR and HL7 in EHR API integration?
HL7 v2 is the older, pipe-delimited messaging standard still widely used in hospital systems for orders, admissions, and lab results. FHIR R4 is the modern RESTful API standard mandated by the ONC Interoperability Rule. New integrations should be built on FHIR, but organizations with legacy systems often need to maintain HL7 v2 connections alongside new FHIR connections.
What is SMART on FHIR and why does it matter?
SMART on FHIR is a security and authorization framework built on OAuth 2.0 that controls how third-party applications access patient data from an EHR. It defines what data an app can request and under what permissions, making it the standard mechanism for safely launching external applications — like patient logistics or care coordination tools — directly within an EHR.
Is FHIR API integration required by law for healthcare providers?
The ONC Interoperability Rule requires certified health IT developers to expose FHIR R4 APIs for patient data access. The CMS Prior Authorization Final Rule extends FHIR API requirements to certain payers, with API compliance dates beginning January 1, 2027. Organizations that block or restrict data access face civil monetary penalties under the information blocking provisions.
How does EHR API integration improve care coordination and patient logistics?
EHR API integration allows platforms outside the EHR — transport coordination, home health, DME systems — to automatically pull current patient data at the moment a care transition is triggered. This eliminates the manual calls, faxes, and data re-entry that slow care handoffs and introduce errors into the process.
What are the biggest challenges of EHR API integration?
The most common challenges are data mapping inconsistencies, API maintenance overhead as EHR vendors release updates, and upfront implementation costs for organizations without dedicated health IT staff. A phased rollout and choosing standards-based FHIR integrations over proprietary connections reduce these risks considerably.
What is USCDI and how does it relate to EHR API integration?
USCDI (United States Core Data for Interoperability) is the federal specification defining the minimum patient data elements — demographics, medications, labs, care plans, and more — that certified EHR systems must expose through their APIs. Verifying that an EHR's API supports the current USCDI version (v6 as of July 2025) is a key step in any integration plan.