Introduction
Every day, millions of patients move through the healthcare system — from emergency scenes to trauma centers, from home to dialysis clinics and back. The logistics behind that movement rarely gets discussed, but its failures are felt immediately: a delayed discharge that backs up the ED, a missed appointment that postpones a diagnosis, a transfer where critical information never arrived.
NEMSIS reported over 60 million EMS activations in 2024 from nearly 15,000 agencies across the country — and that's just emergency transport. Add Medicaid NEMT, interfacility transfers, and in-hospital movement, and the total picture spans tens of millions of additional trips annually.
This post covers the full scope of patient transportation: what it is, the different types involved, why it matters for clinical and operational outcomes, and how modern technology is beginning to address the coordination challenges that make it difficult.
Key Takeaways
- Patient transportation spans everything from a hallway wheelchair push to a cross-state air ambulance transfer
- Delays in transport directly affect length of stay, bed availability, and hospital throughput
- Four distinct transport types exist: emergency, NEMT, inter-facility, and in-facility — each with different staffing, compliance, and acuity requirements
- Coordinating across these transport types is a foundational infrastructure challenge, not a scheduling problem
- Purpose-built platforms are replacing phone-and-fax dispatch with automated, real-time coordination
What Is Patient Transportation?
Patient transportation is the organized movement of patients between or within healthcare settings to ensure they receive the right care at the right time. That definition covers a wider range than most people assume — from an orderly wheeling a patient to radiology, to a flight nurse managing a critical interfacility transfer across two states.
Two main contexts define it:
- In-facility transport — movement within a single hospital or clinic, using wheelchairs and stretchers operated by trained patient transporters
- External patient transport — movement to, from, or between care settings using ground vehicles, aircraft, or specialized medical transport operated by EMTs, paramedics, NEMT drivers, or flight crews
The distinction matters because each context involves different personnel, different regulatory requirements, and different levels of clinical support during transit.
Why It's a Care-Critical Function
Patient transportation isn't a background task. When a patient can't move — whether due to a delayed discharge ride, a missed NEMT pickup, or a slow inter-facility transfer — care is interrupted. Beds stay occupied. Surgical schedules shift. Emergency departments back up.
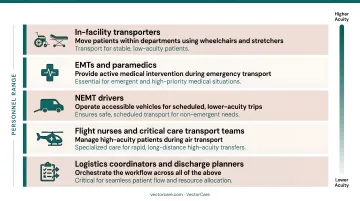
Each failure point has a different cause — and a different person responsible for preventing it. The personnel involved span a wide acuity range:
- In-facility transporters — move patients within departments using wheelchairs and stretchers
- EMTs and paramedics — provide active medical intervention during emergency transport
- NEMT drivers — operate accessible vehicles for scheduled, lower-acuity trips
- Flight nurses and critical care transport teams — manage high-acuity patients during air transport
- Logistics coordinators and discharge planners — orchestrate the workflow across all of the above
That range — from manual transport to critical care flight — is why patient transportation is an infrastructure problem, not just a scheduling one. Coordinating it effectively requires systems that can handle every level of that complexity.
Types of Patient Transportation
Not all patient transportation is the same. The type required depends on the patient's condition, urgency, distance, and the level of medical support needed during transit.
Emergency Medical Transport (EMS/Ambulance)
Emergency transport covers ground ambulances and air medical transport — both rotor-wing (helicopter) and fixed-wing aircraft — dispatched for time-sensitive, life-threatening situations. EMTs or paramedics provide active medical intervention throughout the trip.
A few numbers that frame the scale:
- Ground ambulances account for 98% of all ambulance trips, according to the Health Care Cost Institute
- NEMSIS reported 36.4 million treated-and-transported 911 responses in 2024
- Air medical transport handled an estimated 273,803 rotor-wing and 43,464 fixed-wing transfers in 2021
Emergency transport is governed by strict federal and state regulations, and costs are significantly higher than non-emergency alternatives — the median employer-sponsored insurance base rate for ground ambulance runs around $718, compared to Medicare's $365.
Non-Emergency Medical Transportation (NEMT)
NEMT covers scheduled, non-urgent transport for patients who need a medically appropriate vehicle but not emergency care. Common use cases include:
- Dialysis appointments and recurring outpatient treatments
- Post-discharge follow-ups and specialist visits
- Rehabilitation sessions requiring stretcher or wheelchair-accessible transport
Vehicles range from wheelchair-accessible vans to stretcher vans. NEMT is a federally mandated Medicaid benefit (codified by the Consolidated Appropriations Act of 2021), and approximately 3 to 4 million Medicaid beneficiaries use NEMT annually, according to CMS.
Inter-Facility Transport
Inter-facility transport moves patients between healthcare facilities. The mode — ground ambulance, NEMT, or air transport — depends on patient acuity. Common transfer scenarios include:
- Community hospital to regional trauma center
- ICU to skilled nursing facility or long-term acute care
- Emergency department to inpatient psychiatric unit
This is where coordination complexity is highest. Multiple organizations must communicate in real time, and the consequences of miscommunication are serious. A study of ICU transfers found that 28.5% of transferred patients arrived without documented laboratory analysis, and higher documentation completeness was associated with significantly lower in-hospital mortality.
In-Facility Transport
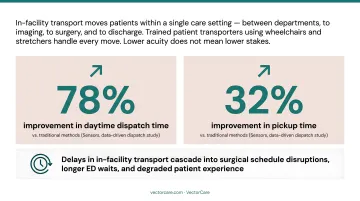
In-facility transport covers movement within a single care setting — between departments, to imaging, to surgery, or to discharge. It's handled by trained patient transporters using wheelchairs and stretchers.
Lower acuity doesn't mean lower stakes. Delays in in-facility transport create bottlenecks that cascade into surgical schedule disruptions, longer ED waits, and degraded patient experience. Research published in Sensors found that data-driven dispatch in patient transport improved daytime dispatch time by 78% and pickup time by 32% compared to traditional methods.
Why Patient Transportation Matters for Healthcare Outcomes
Length of Stay and Hospital Throughput
Every hour a patient waits for a discharge ride, a transfer vehicle, or a post-op transport is an hour of unnecessary bed occupancy. When that delay multiplies across dozens of patients daily, the operational drag compounds fast. Hospital length of stay increased 19% compared to 2019 levels, according to AHA-linked reporting — delayed discharges are a known contributor.
NEMT specifically has a measurable return. CMS's NEMT Report to Congress cites estimates that modern digital NEMT networks can save approximately $268 per member per year compared to traditional coordination models — suggesting that better logistics doesn't just improve operations, it reduces overall costs.
Patient Safety During Transit
Patients in transit are often at their most vulnerable. Poorly coordinated transport — wrong level of care, late arrival, missing handoff information — can directly cause harm. AHRQ PSNet documents errors including wrong patient, wrong destination, and missed medication in transit.
A prospective study of critically ill patients found 294 unique incidents across 455 interhospital transports, with only 1% reported in electronic systems. These aren't rare edge cases — they're a predictable outcome of fragmented, manual coordination.
Equity and Access
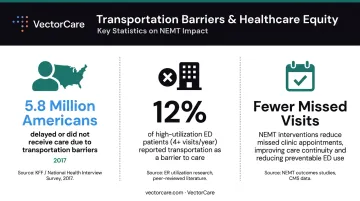
For underserved populations, elderly patients, and people in rural areas, transportation barriers are one of the most consistent obstacles to care. Research published in the Journal of General Internal Medicine found that 5.8 million Americans delayed medical care in 2017 because of transportation barriers. Among adults with four or more ED visits per year, that figure jumped to 12%.
A systematic review found that NEMT interventions for patients with transportation barriers were associated with substantially fewer missed clinic visits — confirming that transportation access is a health outcome issue, not just a convenience issue.
Connection to Broader System Performance
Patient transportation directly affects the metrics hospitals and payers are measured on: readmission rates, time-to-treatment, and discharge efficiency. A delay at any point in the transport chain ripples into quality scores, bed utilization, and reimbursement. That's why logistics coordination has shifted from a scheduling task to a clinical and financial priority.
Key Challenges in Patient Transportation Coordination
Fragmentation Across Too Many Parties
Patient transportation involves dozens of disconnected players — hospitals, NEMT brokers, ambulance companies, air transport services, and home health agencies. Most still communicate via phone, fax, or email, which means errors accumulate, delays compound, and no one has real-time visibility into where a patient is or when they'll arrive.
MACPAC's NEMT review documented beneficiary complaints including late pickups, long hold times, and vehicles not equipped for their needs — problems that trace directly back to coordination failures between disparate organizations.
Acuity Matching Errors
Matching the wrong transport level to a patient's condition is a persistent problem. Sending an ambulance when NEMT is appropriate, or the reverse, carries both clinical and financial consequences. CMS reported a 13.2% improper payment rate for ambulance services in its most recent reporting period, equal to $595 million in projected improper payments. Medical necessity issues accounted for 27.5% of those errors.
HHS OIG separately found $8.7 million in improper Medicare payments for non-emergency ambulance transports to destinations not covered by Medicare. When dispatchers rely on manual judgment rather than decision support tools, these mismatches are difficult to prevent at scale.
Documentation and Compliance Burden
Each transport requires its own administrative stack. Managing this manually pulls nursing staff and discharge planners away from direct care — and creates compliance exposure when gaps occur. Given that insufficient documentation accounts for 63.5% of ambulance services improper payments, the administrative stakes are real.
Documentation requirements per transport typically include:
- Patient records and clinical history
- Consent forms and authorization
- Billing codes and insurance verification
- Regulatory and compliance documentation
Fragmentation, acuity mismatches, and documentation burdens don't exist in isolation — they reinforce each other, making patient transportation coordination one of the most operationally complex functions in healthcare.
Technology's Role in Modern Patient Logistics
From Phone Tag to Automated Workflows
The traditional transport coordination model — phone calls, faxes, manual dispatch boards — creates inherent delays. Modern patient logistics platforms replace that process with automated matching, real-time broadcasting to available providers, and confirmed acceptance in seconds rather than hours.
The operational difference is significant. Before implementing VectorCare, nurses and case managers at one health system spent hours faxing and calling to schedule standing orders for dialysis transport. After implementation, the same workflow — scheduling up to 365 individual trips and broadcasting to local providers — took 3 to 5 minutes.
Real-Time Visibility and EHR Integration
Platforms that connect to electronic health records can automatically pull patient data at the point of a transport request, eliminating duplicate entry and reducing errors. Transport coordinators gain a single view of patient status, transport location, and estimated arrival, rather than managing information across email threads and phone logs.
VectorCare's SMART on FHIR certification enables direct Epic integration, so transport requests can be initiated from within the EHR itself. Most health systems currently lack this connection between where health data lives and where drivers and vehicles operate — and that gap is where coordination breaks down.
VectorCare's A.D.I. in Practice
VectorCare's Automated Dispatching Intelligence (A.D.I.) illustrates what purpose-built infrastructure looks like at scale. Key platform metrics reflect that scale:
- Processes a new transport request every 23 seconds
- Simultaneously broadcasts to credentialed providers across ground, NEMT, and air transport types
- Serves more than 2,500 healthcare facilities nationwide
- Saved customers over 100,000 hours in 2025 alone
The goal isn't just speed. It's replacing reactive, phone-based coordination with proactive, managed infrastructure — so that transport decisions are made on data, not availability of whoever answers the phone.
Frequently Asked Questions
What is the purpose of patient transport?
Patient transport exists to safely move patients to and from the care they need — within facilities, between facilities, or from home — ensuring logistical barriers don't interrupt or delay clinical care. Without it, geography and mobility limitations become clinical barriers.
What are the different types of patient transportation?
The four main types are emergency medical transport (EMS/ambulance), non-emergency medical transportation (NEMT), inter-facility transport, and in-facility transport. Each serves a different level of patient acuity and involves different vehicles, personnel, and regulatory requirements.
What is the difference between emergency and non-emergency patient transport?
Emergency transport — ground ambulance or air — handles urgent, life-threatening situations where active medical care is needed during transit. NEMT is scheduled, lower-acuity transport for patients who need a medically appropriate vehicle but not emergency intervention.
Will Medicare pay for patient transport?
Medicare covers emergency ambulance transport when medically necessary. Some Medicare Advantage plans also offer NEMT as a supplemental benefit. Coverage terms vary by plan, so verify specifics with your insurer or provider.
How much does medical transport cost?
Costs vary widely by type. The 2022 median employer-sponsored insurance ground ambulance base rate was approximately $718 per trip. Air transport is substantially higher — GAO data puts median helicopter transport charges around $36,400. NEMT is far more affordable, though no authoritative national per-trip average is publicly available.
Is patient transport difficult to coordinate?
Yes — it involves real-time coordination across multiple parties, regulatory compliance, acuity matching, and patient safety considerations simultaneously. Platforms like VectorCare tackle this directly through automated dispatching, EHR-integrated data exchange, and unified visibility across transport types — reducing manual coordination tasks by up to 90%.